Integrated High-Risk Pain Management Clinic: Addressing co-morbid pain and depression in high risk chronic opiate use patients

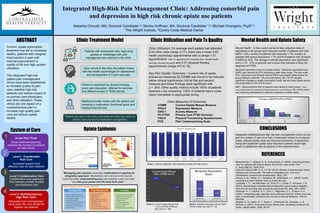
Current opiate prescription treatment has led to increased deaths, patients with marginal improvement in pain with minimal improvement in quality of life and high system utilization. The integrated high-risk patient pain management clinics have been established to increase quality of pain care, stabilize high-risk patients and reduce impact of on primary care physicians and clinic utilization. These clinics are one aspect of a comprehensive plan to increase high quality pain care and reduce opiate deaths. Mental Health – In this current period of data collection rates of depression in all groups were reduced number of patients with mild MDD < 10%, number of patients with moderate < 7%, number of patients with severe depression < 7% and # of patients with all levels of MDD by 23%. The change in sample depression was significant with p =.01. 37% of patients had a score that indicates a likely full diagnosis of PTSD.
Recommended

Recommended
More Related Content
What's hot
What's hot (19)
Similar to Integrated High-Risk Pain Management Clinic: Addressing co-morbid pain and depression in high risk chronic opiate use patients
Similar to Integrated High-Risk Pain Management Clinic: Addressing co-morbid pain and depression in high risk chronic opiate use patients (20)
More from Michael Changaris
More from Michael Changaris (20)
Recently uploaded
Recently uploaded (20)
Integrated High-Risk Pain Management Clinic: Addressing co-morbid pain and depression in high risk chronic opiate use patients
- 1. Current, opiate prescription treatment has led to increased deaths, patients with marginal improvement in pain with minimal improvement in quality of life and high system utilization. The integrated high-risk patient pain management clinics have been established to increase quality of pain care, stabilize high-risk patients and reduce impact of on primary care physicians and clinic utilization. These clinics are one aspect of a comprehensive plan to increase high quality pain care and reduce opiate deaths. Integrated High-Risk Pain Management Clinic: Addressing comorbid pain and depression in high risk chronic opiate use patients Natasha Choudri, MA, Doctoral Candidate1,2; Morley Hoffman, MA, Doctoral Candidate 1,2; Michael Changaris, PsyD1,2 1The Wright Institute, 2Contra Costa Medical Center Clinic Utilization: On average each patient had attended 8.44 clinic visits (range 3-17), there was a mean 5.63 health psychology appointments with a (range 1-31 appointments *note 31 appointments included other mental health services not pain focused) and 3.37 physical therapy appointments (range of 0 to 15). Key Pain Quality Outcomes – Current risk of opiate misuse as measured by COMM was found to be reduced below clinical significance (>9) at first and second measure and these findings were significant with p = .000. Other quality metrics include 100% of patients received u-tox screening, 100% of patients had a cures report completed in appropriate timing. Clinic Measures of Outcomes COMM Current Opiate Misuse Measure PHQ-9 Depression Measure GAD-7 Anxiety Measure PC-PTSD Primary Care PTSD Screener FAQ-5 Physical Functioning Questionnaire PCS Pain Catastrophizing Scale Mental Health – In this current period of data collection rates of depression in all groups were reduced number of patients with mild MDD < 10%, number of patients with moderate < 7%, number of patients with severe depression < 7% and # of patients with all levels of MDD by 23%. The change in sample depression was significant with p =.01. 37% of patients had a score that indicates a likely full diagnosis of PTSD. Morphine Equivalent Dose and Opiate Safety – Morphine equivalent dose (MED) was reduced by 57% indicating a safer dose range. The pain scale Pain, Enjoyment and General Activity (PEG) was largely stable across the group between initial (M = 23) and post testing (M = 22.07) despite significant changes in opiate prescription levels. Narcan nasal opiate rescue was prescribed to 40% of this cohort. MAT – Buprenorphine 40% of patients were taking at chart review, (* Note some patients received methadone and buprenorphine for pain treatment), 3% of this cohort was receiving methadone for addiction treatment in offsite center. Integrated multidisciplinary high risk pain management clinics as one part of a system of care have had a meaningful impact on increased safety, reduced opiate dose and improved symptoms of depression. Along with significant opiate dose reductions patients report high levels of satisfaction with all aspects of the treatment team. Clinic Treatment Model Opiate Epidemic Bodenheimer, T., Wagner, E. H., & Grumbach, K. (2002). Improving primary care for patients with chronic illness: the chronic care model, Part 2. Jama,288(15), 1909-1914. Carri-Ann Gibson MD, D. A. A. P. M. (2012). Review of posttraumatic stress disorder and chronic pain: The path to integrated care. Journal of rehabilitation research and development, 49(5), 753. Krause, K. M., Pollak, K. I., Gradison, M., & Michener, J. L. (2009). Family physicians as team leaders:“time” to share the care. Lambeek, L. C., van Mechelen, W., Knol, D. L., Loisel, P., & Anema, J. R. (2010). Randomised controlled trial of integrated care to reduce disability from chronic low back pain in working and private life. Bmj, 340, c1035. Sherman, K. J., Cherkin, D. C., Erro, J., Miglioretti, D. L., & Deyo, R. A. (2005). Comparing yoga, exercise, and a self-care book for chronic low back pain: a randomized, controlled trial. Annals of Internal Medicine, 143(12), 849-856. Wagner, E. H., Austin, B. T., Davis, C., Hindmarsh, M., Schaefer, J., & Bonomi, A. (2001). Improving chronic illness care: translating evidence into action. Health affairs, 20(6), 64-78. CONCLUSIONS Mental Health and Opiate SafetyClinic Utilization and Pain Tx Quality REFERENCES Chart 2. Current Opiate Misuse Risk > 9 is Low Risk of Misuse, Sig. t-test P = .000 Chart 3. Morphine Equivalent Dose >60% Clinical Impact sig t-test P = .02 Chart 1. Patient satisfaction with treatment provided (40 data points) ABSTRACT Upon arrival in the clinic the patient meets with the health psychologist for assessment and development of 5 part care plan. Patients with behavioral risks, high-dose opiates or challenges with pain management are referred to the clinic. Patient is assessed by physical therapy, given pain education, referred for services and offered access to TENS device. Medical provider meets with the patient and develops a medication, functional goals and biopsychosocial plan. 4.83 4.75 4.90 4.80 4.89 4.70 4.65 4.90 4.95 4.92 0.00 0.50 1.00 1.50 2.00 2.50 3.00 3.50 4.00 4.50 5.00 Wait time? Your needs met? Physician Care? Physical Therapist Care? Health Psychology Care? Information about condition? Pain management program? How did staff treat you? Nursing staff? Your appointment today? Patient Satisfaction 99.80 42.22 MORPHINE EQUIVILANT DOSE 1 MORPHINE EQUIVILANT DOSE 2 Morphine Equivalent Dose 10.96 6.50 0.00 2.00 4.00 6.00 8.00 10.00 12.00 1 2 Current Opiate Misuse Risk: COMM Score“Managing pain requires more then medications it requires an integrative approach. Medications are one tool in the tool kit. Learning skills, understanding pain and building a plan can help you take your power and life back from pain.” Level 2 Collaborative Care Collaborative care approach that reduces provider burden and increases care System of Care Patients are seen in the clinic until stable and then they return to primary care provider for medication management. Level 3 Multidisciplinary High Risk Team Integrated pain management using share the care model for highest risk patients Level I - Coordinated Pain Care Increased support and effective care for pain patients Acute Pain Track Early treatment planning reduces the number of patients on risky doses 1 2 3 4 MDD All PHQ-9 > 10 MDD Mild (10-15) MDD Moderate (15-20) MDD Severe (20+) PHQ-9 Pre 60% 40% 20% 7% PHQ-9 Post 37% 30% 13% 0% 60% 40% 20% 7% 37% 30% 13% 0% PercentofPatientswithMDD Change in MDD Pre/Post PHQ-9