1. Impact
of
livingwell
CARES
On-‐Site
Care
Coordina8on
Program
on
Diabetes
Health
Outcomes
Kathryn D. Cannon, MBS; Eileen Blake, MPH; E. Anne Peterson, MD, MPH; Vivian Green, PhD
Public Health Program, PONCE HEALTH SCIENCES UNIVERSITY, PONCE RESEARCH
INSTITUTE, Ponce, Puerto Rico
INTRODUCTION
PURPOSE
METHODS
Diabetes is a leading contributor to premature mortality in
the United States
• 382 million with disease and has resulted in 1.4 million deaths
o 90% with Type 2 Diabetes ~ 3.3% of total population
• Diabetes self-management support has been shown to improve
health outcomes
• Yale New Haven Health System livingwell CARES (LWC)
program began enrolling employees with chronic diseases in a
health intervention program in 2012
• Care coordination programs may be effective in improving
health outcomes among individuals with chronic diseases,
such as diabetes.
1. Assess the impact of a chronic disease management program
on a population of diabetic patients.
• Impact of blood pressure (BP), body mass index
(BMI), low density lipoprotein (LDL), and hemoglobin A1c
(HbA1c) levels and overall cost related to care of these
patients
2. Explore other relevant program outcomes
• Assess overall patient satisfaction and determine
opportunities to expand to other chronic diseases
Study Subjects:
• Participants were chronic disease patients treated by Yale
New Haven Health System
• Participation restricted to
o Yale New Haven Health System employees and spouses
o Individuals with diabetes
o Enrolled in the program between April 2012 and April
2013
• Intervention group: diabetic individuals who were offered and
accepted enrollment in the livingwell CARES (LWC) Program
• Control group: diabetic individuals from the YNHH
diabetes registry
Data collection:
• Duration: April 2012 – April 2014
• HbA1c, LDL, BMI, BP, and health care cost records obtained
from Epic (YNHH EMR) and Advisory Board (utilization
aggregate) data using medical record number (MRN)
as unique patient identifier
• Crystal Reports generated from Epic and exported as
Microsoft Excel documents for statistical analysis
• A total of 1,263 patient records were collected
• Patients signed informed consent upon enrollment
in livingwell CARES program
RESULTS
CONCLUSIONS
• Preliminary analysis of pilot livingwell CARE program
reveal positive health outcomes in diabetic patients
in comparison to usual care patients
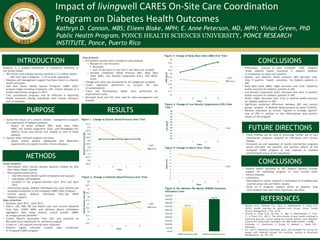
• Systolic and diastolic blood pressure (BP): decrease over
time à positive health outcomes for diabetic patients in
LWC
• Body Mass Index (BMI): slight decrease over time àpositive
health outcome for diabetic patients in LWC
• Low Density Lipoprotein (LDL): decrease over time à positive
health outcome for diabetic patients in LWC
• HbA1c: slight decrease over time à positive health outcome
for diabetic patients in LWC
• Significant statistical difference between LWC and control
groups present in diastolic blood pressure (p-value= 0.0434)
• Patients expressed an overall “agreed or strongly agreed”
rate of 95% in relation to the effectiveness and positive
impact of the program
FUTURE DIRECTIONS
• These findings can be used to encourage further use of care
coordination programs targeted at individuals with chronic
disease.
• Increased use and expansion of health intervention programs
would elucidate the benefits and positive effects of the
livingwell CARES program to may improve or stabilize
overall health status of the population.
CONCLUSIONS
• Positive health outcomes of LWC diabetic patients provide
support for expanding program to treat include other
chronic diseases
• Limitations:
o Retrospective review resulted in limitations on available data
(control group LDL and HbA1c values)
o Early on in program, analysis serves as baseline, long
term analysis may show more significant outcomes
REFERENCES
• Bennett, H.D., Coleman, E.A., Parry, C., Bodenheimer, T., Chen, E.H.
(2010). Health coaching for patients with chronic illness. Family
Practice Management, 17(5), 24-29.
• Ghorob, A., Vivas, M.M., De Vore, D., Ngo, V., Bodenheimer, T., Chen,
E., & Thom, D.H. (2011). The effectiveness of peer health coaching in
improving glycemic control among low-income patients with diabetes:
protocol for randomized controlled trial. BMC Public Health, 11(208).
• Schneider, J.I., Hashizume, J., Sreang, H., Maetani, L., Ozaki, R.R.,
Watanabe,
• D.L. (2011). Identifying challenges, goals, and strategies for success for
people with diabetes through life coaching. Journal of Vocational
Rehabilitation, 34, 129– 139.
Data Analysis:
• 637 patient records were included in data analysis.
o Reasons for non-inclusion:
§ Deceased
§ Lack of lab value or less than 3 lab values for variable
o Variable categories: Blood Pressure (BP), Body Mass
Index (BMI), Low Density Lipoprotein (LDL), and HbA1c
levels
• Change over time was calculated for all categorical variables
• Linear regression performed to account for lack
of randomization
• T-test and Parsimonious Model were performed for
improvement score
• Microsoft Excel and SAS were used for data management and
analysis
31
31.5
32
32.5
33
33.5
34
34.5
35
35.5
36
1
2
3
4
BMI
kg/m2
Years
LWC
Control
Figure 3: Change of Body Mass Index (BMI) Over Time
Figure 4: Change of Low Density Lipoproteins (LDL) Over
Time *
80
81
82
83
84
85
86
87
88
89
90
1
2
3
4
LDL
mg/dL
Years
LWC
0
1
2
3
4
5
6
7
8
9
1
2
3
4
HbA1c
(%)
Years
LWC
Figure 5: Change of HbA1c Over Time*
$339.40
$449.93
$0.00
$50.00
$100.00
$150.00
$200.00
$250.00
$300.00
$350.00
$400.00
$450.00
$500.00
YNHH
Employees
LWC
YNHH
Employees
Overall
Figure 6: Per-Member-Per-Month (PMPM) Employee
Utilization Costs
125.5
126
126.5
127
127.5
128
128.5
129
129.5
130
130.5
131
131.5
1
2
3
4
Blood
Pressure
(mm
Hg)
Years
LWC
Control
Figure 1. Change in Systolic Blood Pressure Over Time
74.5
75
75.5
76
76.5
77
77.5
78
78.5
79
79.5
80
1
2
3
4
Blood
Pressure
(mm
Hg)
Years
LWC
Control
Figure 2. Change in Diastolic Blood Pressure Over Time