
Recommended
More Related Content
What's hot
What's hot (20)
Similar to CREST Syndrome
Similar to CREST Syndrome (20)
Recently uploaded
Recently uploaded (20)
CREST Syndrome
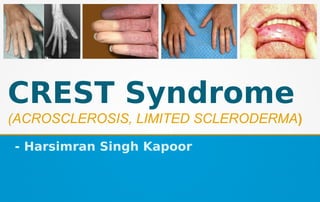
- 1. CREST Syndrome (ACROSCLEROSIS, LIMITED SCLERODERMA) - Harsimran Singh Kapoor
- 2. INTRODUCTION It is an uncommon condition that may be considered a relatively mild variant of systemic sclerosis. ● CREST syndrome, also known as the limited cutaneous form of systemic sclerosis (lcSSc), is a multisystem connective tissue disorder. The symptoms involved in CREST syndrome are associated with the generalized form of the disease Systemic sclerosis (scleroderma).
- 3. CREST is an acronym for the clinical features that are seen in a patient with this disease. The "C" stands for Calcinosis, where calcium deposits form under the skin on the fingers or other areas of the body. The "R", stands for Raynaud's phenomenon, spasm of blood vessels in the fingers or toes in response to cold or stress. The "E" represents Esophageal dysmotility, which can cause difficulty in swallowing. The "S" is for Sclerodactyly, tightening of the skin causing the fingers to bend. The letter "T" is for Telangiectasia, dilated vessels on the skin of the fingers, face, or inside of the mouth.
- 4. Scleroderma, derived from the Greek words for hard and skin, is used to describe a group of clinical disorders characterized by thickening and fibrosis of the skin. There are two main forms, progressive systemic sclerosis (PSS) and localized sclerodema. PSS is further divided into limited cutaneous scleroderma (also called CREST syndrome) and diffuse cutaneous scleroderma. ● Patients with limited scleroderma often have a long history of Raynaud’s phenomenon before the appearance of other symptoms. ● They have skin thickening limited to the hands and frequently have problems with digital ulcers and esophageal dysmotility.
- 5. ETIOPATHOGENSIS The etiology is unclear, but the pathogenesis is characterized by vascular damage and an accumulation of collagen and other extracellular matrix components at involved sites. ● Biopsies of the skin in early stages demonstrate bundles of collagen in the lower dermis and upper subcutaneum in association with perivascular and interstitial mononuclear cell infiltrates. ● The inflammatory process precedes the deposition of collagen.
- 6. ● Once in the tissue, T cells drive processes through secretion of cytokines such as IL-4 and IL-13 that result in vasculopathy and fibrosis. ● These cytokines induce fibroblast production of transforming growth factor b1, which is the main profibrotic cytokine in PSS. ● As the disease progresses, the rete pegs are lost and the epidermis thins. ● Unregulated collagen deposition is a hallmark of this disease. Cultured fibroblasts from patients synthesize more collagen in vitro that is structurally normal, although collagen degradation pathways appear to be normal.
- 7. ● The excess collagen narrows small arteries and changes the microvasculature in early stages of the disease, causing eventual pulmonary hypertension, renal disease, myocardial dysfunction and digital gangrene. ● There appears to be a small genetic predisposition to PSS. ● ● Environmental exposure to pesticides, benzene derivatives, and silica has been linked to the development of scleroderma-like conditions in miners and stonemasons. ● Viral triggers, such as parvovirus B19, are proposed.
- 8. CLINICAL MANIFESTATIONS The characteristic signs may not appear synchronously but instead may develop over a period of months to years. 1. Calcinosis cutis - ● It occurs in the form of movable, nontender, subcutaneous nodules, 0.5 to 2.0 cm in size, which are usually multiple. ● Larger, more numerous or superficial calcifications may occasionally become bothersome and require removal.
- 9. 2. Raynaud’s phenomenon - It may be observed when a person’s hands or feet are exposed to cold temperatures. ● The initial clinical sign is a dramatic blanching of the digits, which appear dead- white in color as a result of severe vasospasm. ● A few minutes later, the affected extremity takes on a bluish color because of venous stasis.
- 10. ● After warming, increased blood flow results in a dusky- red hue with the return of hyperemic blood flow. ● This may be accompanied by varying degrees of throbbing pain. ● When extreme and frequent, this phenomenon can lead to digital ulcerations, gangrene, or amputation. Ulceration can predispose to chronic infections of the involved site.
- 11. 3. Esophageal dysfunction - It is caused by abnormal collagen deposition in the esophageal submucosa, may not be noticeable in the early phases of CREST syndrome. It may present as a sensation of food getting stuck (dysphagia) in the mid- or lower esophagus, atypical chest pain, or cough. ● People often state they must drink liquids to swallow solid food. This motility problem results from atrophy of the gastrointestinal tract wall smooth muscle. ● This change may occur with or without pathologic evidence of significant tissue fibrosis. ● Often the subtle initial signs of this problem must be demonstrated by barium swallow radiologic studies.
- 12. 4. Sclerodactyly - Sclerodactyly of CREST syndrome is rather remarkable. The fingers become stiff and the skintakes on a smooth, shiny appearance. Often the fingers undergo permanent flexure, resulting in a characteristic “claw” deformity. ● Though it is the most easily recognizable manifestation, it is not prominent in all patients. ● Thickening generally only involves the skin of the fingers distal to the metacarpophalangeal joints in CREST.
- 13. ● Early in the course of disease, the skin may appear edematous and inflamed. Eventually, dermal fibroblasts overproduce extracellular matrix leading to increased tissue collagen deposition in the skin. ● Collagen cross-linking then causes a progressive skin tightening. ● Digital ischemic ulcers commonly form on the distal fingers in 30- 50% of patients. ● As with systemic sclerosis, this change is due to abnormal deposition of collagen within the dermis in these areas.
- 14. 5. Telangiectasias - Telangiectasis in this syndrome are similar to those seen in hereditary hemorrhagic telangiectasia (HHT). ● As with that condition, significant bleeding from the superficial dilated capillaries may occur. ● The facial skin and the vermilion zone of the lips are commonly affected.
- 15. ● Marked telengiectasis (dilated capillaries) occur on the skin of the face, the palmar surface of the hands, and the mucous membranes. ● Telangiectasias tend to be more numerous in people with other scleroderma related vascular disease (i.e., pulmonary arterial hypertension). The number of telangiectasias and the sites involved tend to increase over time.
- 16. Other symptoms of CREST syndrome can be..... - exhaustion, - weakness, - difficulties with breathing, - pain in hands and feet, - dizziness and - badly healing wounds. Patients with syndrome commonly induce pulmonary artery hypertension which may result in cor pulmonale (heart failure due to increased pulmonary artery pressure).
- 17. ORAL MANIFESTATIONS The clinical signs of scleroderma of the mouth and jaws are consistent with findings elsewhere in the body. - The lips become rigid and the oral aperture narrows considerably. - Skin folds are lost around the mouth, giving a mask like appearance to the face. - The tongue can also become hard and rigid, making speaking and swallowing difficult. Involvement of the esophagus may cause dysphagia.
- 18. ● Oral telangiectasia is most commonly observed on the hard palate and the lips. ● When fibrosis involves the muscles of mastication, mandibular resorption can occur either the angle of the mandible, the condylar heads, the coronoid process, or the digastric region. ● Mandibular movement may be restricted by muscular fibrosis.
- 19. DIAGNOSIS CREST is not easily diagnosed as it closely mimics symptoms of other connective tissue and autoimmune diseases. Diagnosis is usually given when a patient presents two or more of the five major clinical symptoms. ● In these cases, laboratory studies directed at identifying anticentromere (ACA) ; antitopoisomerase I (anti-topo I); anti–ribonucleic acid (RNA) polymerase I/III; and anti-Th/To antibodies may be useful, because these tests are relatively specific for CREST syndrome.
- 20. ● Circulating ANAs are present in >90% of the patients. ● Other non specific autoantibodies which can be detected in serum, include anti-PM-Scl, anti- U3RNP, and anti- U1RNP. ● Autoantibodies appear to have prognostic value for patients. ACAs are strongly associated with slowly progressive, limited disease, whereas anti-topo I and anti- RNA polymerase I/III are found more frequently in patients with progressive and diffuse disease. ● Additionally, skin biopsies can be given to help confirm a diagnosis.
- 21. ● Other abnormal laboratory findings include anemia, an elevated erythrocyte sedimentation rate, and hypergammaglobulinemia. ● The diagnosis is made from the presence of characteristic cutaneous skin thickening in association with Raynaud’s phenomena. ● Proximal sclerodermatous skin changes (proximal to the metacarpophalangeal joints) in the presence of two minor criteria (sclerodactyly, digital pitting scars of fingertips or loss of the distal finger pad, or bibasilar pulmonary fibrosis).
- 23. ● Classic dental radiographic findings such as extreme widening of the periodontal ligament, two to four times normal thickness. ● Bone resorption of the angle of the mandibular ramus (usually bilaterally), Partial or complete resorption of condyles and/or coronoid processes of the mandible has been reported. ● Other characteristic radiographic findings include calcinosis of the soft tissues around the jaws.
- 24. HISTOPATHOLOGICAL FINDINGS The histopathologic findings in CREST syndrome are similar, although milder, to those seen in systemic sclerosis. Microscopic examination of tissue involved shows diffuse deposition of dense collagen within and around the normal structures. This abnormal collagen replaces and destroys the normal tissue, causing the loss of normal tissue function. Superficial dilated capillaries are observed if a telangiectatic vessel is included in the biopsy specimen.
- 25. ● thickening and hyalinization of the collagen fibers in the skin, ● loss of dermal appendages, particularly the sweat glands, ● atrophy of the epithelium with loss of rete pegs and increased melanin pigmentation. ● Subcutaneous fat disappears and the walls of the blood vessels become sclerotic. It is characterized microscopically by -
- 26. ● There is an increase in PAS-positive, diastase-resistant material present in the areas of the homogeneous collagen. ● Mucous membrane changes are similar to those occurring in the skin. The microscopic changes in the periodontal ligament consist of a widening due to an increase of collagen and oxytalan fibers as well as an appearance of hyalinization and sclerosis of collagen with a diminution in the number of connective tissue cells usually found.
- 27. MANAGEMENT The treatment of patients with CREST syndrome is essentially the same as that of those with systemic sclerosis. Because CREST syndrome usually is not as severe, so the treatment does not have to be as aggressive. Unfortunately, many of the recommended treatments have not been examined in controlled trials, and the natural waxing and waning course of the disease makes it difficult to assess the effectiveness of a given treatment in an open- label trial.
- 28. ● Systemic medications such as penicillamine, are prescribed in an attempt to inhibit collagen production. ● A recent double-blind study, however, showed no difference in measured patient outcomes with high-dose versus low-dose penicillamine, suggesting that perhaps this medication has limited efficacy. ● Surprisingly, corticosteroids are of a little benefit. ● Extracorporeal photochemotherapy has shown some beneficial effect on the skin lesions; however, no improvement of the pulmonary function tests is observed.
- 29. ● Other management strategies directed at controlling symptoms. Such as esophageal dilation to temporarily correct dysfunction and dysphagia. ● Calcium channel blocking agents help to increase peripheral blood flow and lessen the symptoms of Raynaud’s phenomenon, but many patients can reduce episodes by keeping warm (especially their hands and feet) or by stopping cigarette smoking. ● Angiotensin-converting enzyme (ACE) inhibitors often effectively control hypertension if kidney involvement is prominent.
- 30. ● Physical therapy - Stretching exercises are important to help prevent loss of mobility in stiff & painful joints. Facial exercises can help keep your face and mouth flexible. It helps to maintain flexibility and strength. Surgery may be needed for certain problems, such as: ● Calcium deposits - Large or painful calcium deposits are sometimes surgically removed. ● Red spots or lines - Laser surgery can reduce the appearance of red spots or lines caused by swollen blood vessels near the surface of the skin.
- 31. DENTAL MANGEMENT The most common problem in the dental treatment of patients is the physical limitation caused by the narrowing of the oral aperture and rigidity of the tongue. Procedures such as molar endodontics, prosthetics and restorative procedures in the posterior portions of the mouth become difficult and the dental treatment plan may sometimes need to be altered because of the physical problem of access.
- 32. ● The oral opening may be increased an average of 5 mm by stretching exercises. ● One particularly effective technique is the use of an increasing number of tongue blades between the posterior teeth to stretch the facial tissues. ● Mechanical stretching devices are available. If these approaches are insufficient, a bilateral commissurotomy may be necessary. ● Collapsible dental appliances with special hinges have been made to facilitate the insertion and removal of dentures.
- 33. ● Microstomia and inelastic soft tissue also hamper the maintenance of good oral hygiene. ● Patients have a decreased ability to manipulate a toothbrush as a result of sclerotic changes in the fingers and hands. ● Caries and plaque were associated with decreasing dexterity and strength. ● Customized toothbrush handles should be provided for patients who cannot grip an ordinary toothbrush.
- 34. ● Surgical correction of open bite associated with condylar resorption has been described. ● Patients with extensive resorption of the angle of the mandible are at risk of developing pathologic fractures from minor trauma, including dental extractions. When treating a patient, the extent of the heart, lung, or kidney involvement should be considered, and appropriate alterations should be made before, during and after treatment.
- 35. PROGNOSIS Although the prognosis for this condition is much better than that for systemic sclerosis, patients should be monitored for an increased risk of developing pulmonary hypertension or primary biliary cirrhosis, generally more than 10 years after the initial diagnosis. If the heart is affected, then the prognosis is particularly poor, most patients die because of pulmonary involvement. Overall survival figures are difficult to calculate because of a variety of factors, including the rarity of the disease, the inherent variability of its natural course and the variation in treatments provided at medical centers around the world.
- 36. THANK YOU !