
Empfohlen
Weitere ähnliche Inhalte
Ähnlich wie nmj.pptx
Ähnlich wie nmj.pptx (20)
Kürzlich hochgeladen
Kürzlich hochgeladen (20)
nmj.pptx
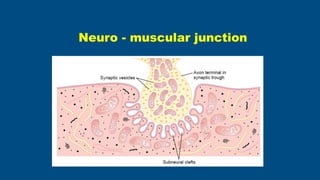
- 1. Neuro - muscular junction
- 2. • To draw the schematic diagram of Neuro-muscular junction • To describe the events of Neuromuscular transmission • Classify neuromuscular blockers & give mechanism of action • Disorders of neuromuscular junction Learning objectives
- 3. • Neuro-muscular junction/ Myoneural junction • Junction between Motor neuron & Muscle fibre • Action potential from nerve is transmitted to muscle through this junction Introduction
- 4. • Terminal button • Presynaptic membrane • Synaptic cleft • Postsynaptic membrane Structure
- 5. • Neuron innervating skeletal muscle fibre –Motor Neurons • Near muscle fibre it looses its myelin sheath & divides into axon terminals • Each terminal is expanded at its tip to form Synaptic Knob/Terminal Button) Presynaptic portion- Axon terminal
- 6. • The motor neuron its axon, its terminal with muscle fibre it supplies –form MOTORUNIT • Terminal button lies in a groove-Synaptic Trough • Vesicles gather at specific points –Active Zones–Membrane at active zone modified to form DenseBars–contains numerous voltage gated Ca channels Presynaptic portion- Axon terminal
- 7. • 50-100 nmwide • Filled with extracellular fluid • Contains acetyl- choline- esterase • It hydrolyses Ach into Acetic acid & Choline Synaptic cleft
- 8. • It’s a part of sarcolemma • Several folds JunctionalFolds increases membrane surface area • Contains Ach-receptors • voltage gatedNachannels Post synaptic membrane
- 9. • Nicotinic type • 15-40 millions/end plate • Chemically gated ion channels • Contains voltage gated Na channels& allow passage of only Cations Acetylcholine receptors
- 10. • Def–Transmission of impulses from motor neuron to skeletal muscle fibre. • Mechanism 3 parts • Presynaptic events • Synaptic events • Post synaptic events. Neuromuscular transmission
- 11. • MainPurpose–To release acetyl choline into synaptic cleft • Steps – • Action potential arrive at axon terminal & Depolarize membrane of terminal button • Activate & open voltage gated Cachannels-Ca influx – increases movements of Microtubules & Microfilamants- causes migration of Neurotransmitter vesicles to pre-synaptic membrane - DOCKING • Release acetylcholine into cleft by Exocytosis Presynaptic events
- 12. • Quantal Release • One vesicle of acetyl choline –Quanta • Process of release of 1 vesicle is Quantal Release • SirKatz,Euler & Axelrod received Nobel prize in 1970 for Quantal release phenomenon Presynaptic movements
- 13. • Binding of acetylcholine to receptors at post synaptic membrane • Onthe way some are hydrolyzed by AChE& remaining act on receptors Events at synaptic cleft
- 14. • Generate Action Potential in sarcolemma • ACh diffuses into cleft & bind with post- synaptic ACh receptors • ACh Gated Ion Channels • 5 sub uints • When 2 molecules are attached conformational change occurs in tubular channels & open it & increases Na influx Post synaptic membrane events
- 15. • RMPof postsynapticmembrane is -80to -90 mV • Influx of Nachannels causes local positive potential change –END PLATE POTENTIAL • It’slocalized,Non-Propogated,Doesnotobey All orNoneLaw • Butwhen critical level of -60mvreached triggers action potential in muscle fibre in both direction End plate potential
- 16. EPP • Only 6 vesicles are required for activation from -90 to -65mv • Each nerve impulse releases 60-125 Ach vesicles • Every vesicle has 10,000 molecules of Ach • 10 fold safety factor • Action potential is always generated
- 17. • At rest, small quantity of acetyl choline are released from nerve terminal • Each vesicle release produces weak end plate potential about 0.5mv–MiniatureEnd Plate Potential Miniature end plate potential
- 18. • Within 1 msby 2ways • Mostly destroyed by Ach-estarase in synaptic cleft • Remaining Diffuses Out of synaptic space & no longer available for action • Reuptake by exchanger - Reused Removal by ACh esterase
- 20. MyastheniaGravis AutoImmune disease Anti bodies are produced against Acetylcholine Receptors & destroy these channels Disorders of NMJ
- 21. • So acetyl choline released will not produceadequate endplate potential & excite muscle fibre • So patient dies of paralysis of Respiratory Muscles Myasthenia gravis
- 22. Treatment • Ameliorated for several hours by administering neostigmine • Anticholinesterase drug • Larger than normal amounts of ACh accumulate in the synaptic space • Within minutes, some of these paralyzed people can begin to function almost normally
- 23. • Lambert-Eaton Syndrome • Anti bodies are produced against calciumchannels present on pre- synaptic membrane • Ca influx decrease & decreases release of acetyl choline Disorders of NMJ
- 24. Myasthenia gravis LEMS Antibodies against Nicotinic receptor for ACh in the muscle Antibodies against Ca channels in the nerve Starts at eyes and moves down Starts at extremities Weakness worsens with activity Weakness improves with activity Associated with tumours of thymus Associated with Ca lung Tt = ACh esterase inhibitor Tt = Aminopyriridines
- 26. What is the rationale behind the use of Calabar bean as a lie detector by some native tribes of West Africa? • Calabar bean - physostigmine, an AChE inhibitor • innocent- consumes rapidly • local gastric irritation (possibly due to accumulation of ACh at parasympathetic postganglionic nerve endings in the stomach) vomits • guilty - scared & apprehensive , small sips • suffers less gastric irritation, does not vomit, in intestines gets absorbed
- 27. Summary
- 29. • Neuromuscular Blockers– this block neuromuscular transmission at junction. • Curare • Bungarotoxin • Succinylcholine and carbamylcholine • Botulinum toxin Drugs affecting NMJ
- 30. • Curare–active principle D- Tubocurarine (Cobra) • Block by combine with Ach-receptors • So Ach cannot act on receptors & No End PlatePotential develop • So these are receptor blockers Neuromuscular blockers
- 31. • Bungarotoxin– • Venomof deadly snake Krait • Also block N-Mjunction by combiningwith acetylcholine receptors Neuromuscular blockers
- 32. • Succinylcholine & Carbamylcholine –act like acetyl choline & Depolarizes post synaptic membrane • But these are not destroyed by cholinesterase –so muscle remain in depolarized state for a long time • So these block Myoneural junction by keeping the muscle in depolarized state Neuromuscular blockers
- 33. • BotulinumToxin –derived from bacteria Clostridium Botulinum • Block the junction by preventing the Release OfAcetyl Cholinefrom terminal button Neuromuscular blockers
- 34. • Drugs having acetylcholine like action- • Methacholine, Carbachol & Nicotin • But these are either not destroyed or destroyed very slowly by acetylcholinesterase so causes repeated stimulation & continuous action of muscle –Muscle spasm Neuromuscular stimulators
- 35. • Drugs that Inactivate the enzyme Cholinesterase (Anticholinesterase) –Neostigmine, Physostigmine & Disopropylflurophosphate (DFP) • So it leads to repeated stimulation & continuous action of muscle. E.g –Laryngeal Spasm Neuromuscular stimulators