
Recommended
More Related Content
What's hot
What's hot (20)
Similar to Club foot
Similar to Club foot (20)
Recently uploaded
Recently uploaded (20)
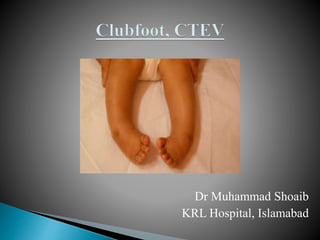
Club foot
- 1. Dr Muhammad Shoaib KRL Hospital, Islamabad
- 2. The term Clubfoot refers to a foot deformity characterized by equinus of the hindfoot and adduction of the midfoot and forefoot with varus through the subtalar joint complex.
- 3. HISTORY OF CLUB FOOT
- 7. Dr Ontonio Scarpa, an Italian surgeon has great contributions in the conservative management of Club Foot and devised a First Club Foot Correction Clamp
- 8. In 1831, surgeon Stromyer first time gave the idea of per cutaneous tenotomy of Tendo Achilles in the out patient clinics as a safe procedure for the correction of Equines of the foot
- 11. Congenital: ◦ Present since birth. ◦ Associated with spina bifida. ◦ Bilateral. ◦ Skin, subcutaneous tissue & muscles normal. ◦ Transverse crease present. ◦ Bones normal.
- 12. Acquired: ◦ Not present since birth. ◦ Due to polio, cerebral palsy etc. ◦ Unilateral. ◦ Tropic changes in skin, muscle flaccid or spastic. ◦ No transverse crease. ◦ Bones are thinner.
- 13. Commonest congenital foot deformity in children. Incidence 1.2/1000 live births. 2-3 times more common in boys than girls. 50 % bilateral. 10 % family history of clubfoot (CTEV).
- 14. Osseous Type: Associated with absence of tibia & fibula. Muscular Type: Arthrogryposis. Neuropathic Type: Due to spina bifida. Idiopathic Type: No apparent cause. Various theories proposed.
- 15. Turco’s: Medial displacement of navicular & calcaneum around talus. Brockman’s: Congenital atresia of talonavicular joint. Mc-Kay’s: Three-dimensional bony deformity of subtalar complex. Intrauterine: Compression by malposition of fetus in utero. Genetic. Germ Plasm Theory: Primary germ plasm defect in talus with subsequent soft tissue changes.
- 16. Soft Tissue Theory: Primary soft tissue defect with secondary bony changes. Prenatal Muscle Imbalance Theory: Weak pronators and overacting extensors and invertors. Herzenberg: Talar neck is internally rotated and talar body is externally rotated relative to ankle mortise.
- 18. 1. Talocalcaneus joint 2. Talocalcaneonaviculer joint 3. Calcanocuboid joint
- 22. 1. Calf is smaller - Shorter and smaller muscle tendon unit of Triceps surae (= Gastrocnemius, Soleus, Plantaris), Tibialis posterior and toe flexor
- 23. 2. Hind foot Equinus - Severe Plantar flexion in the ankle joint. - High Calcaneus (not in the heel pad). - Talus in severe Flexion
- 24. 3. Heel in Varus - Supination and Adduction of the Calcaneus. - Calcaneus is locked under the Talus.
- 25. 4. Inversion of the Mid foot (Inversion = Plantar flexion +Add + Sup) - Navicular is medially displaced, adducted and supinated in relation to the Talus. - Navicular articulates only with the medial part of the head of the Talus.
- 26. 5. Cavus Increase in the height of the medial arch of the foot
- 27. 6. Metatarsal I is more in Plantar flexion than the rest of the Metatarsals
- 28. 7. Clubfoot is smaller than a normal foot.
- 29. Structures contracted on medial side: ◦ 3 muscles AHL TP FHL ◦ 3 ligaments Deltoid Spring Plantar ◦ 3 capsules Subtalar Tarsal Tarsometatarsal
- 30. Structures contracted on posterior side: ◦ 2 muscles Tibialis posterior Tendo-Achilles ◦ 2 ligaments Talofibular Calcaneofibular ◦ 2 capsules Ankle joint Subtalar joint
- 31. Structures contracted on anterior side: ◦ 1 muscle Tibialis anterior if inserted abnormally ◦ 1 ligament Superior peroneal retinacula ◦ 1 capsule Calcaneocuboid joint
- 33. Equinus of heel Hindfoot varus Midfoot cavus Forefoot adduction Internal tibial torsion
- 34. Foot size is decreased to 50%. Medial border is concave, lateral border is convex. Froefoot is plantarflexed upon hindfoot. Skin is stretched over the dorsum of the foot.
- 35. Callosities over dorsum of the foot. Stumbling gait. Hypotrophic anterior tibial atrery. Atrophy of muscles in anterior or posterior compartments of leg.
- 36. Degeneration of joints. Fusion of joints.
- 38. Detects internal tibial torsion. Child is made to sit on a table with both lower limbshanging from the edge.
- 39. A line drawn from centre of patella to tibial tubercle when extended down should cut the foot at 1st or 2nd intermetatarsal space. In CTEV with medial rotation of tibia it cuts 4th or 5th space.
- 40. Detects muscle imbalance in an infant who can not obey commands. Medial Scratch Test: when medial sole is scratched, foot everts. This tests peroneals. Latearl Scratch Test: when lateral sole is scratched, foot inverts. This tests invertors.
- 42. Four parameters are assessed on the basis of their reducibility with gentle manipulation as measured with a handheld goniometer
- 43. 1. Equinus deviation in the sagittal plane 2. Varus deviation in the frontal plane 3. Derotation of the calcaneopedal block in the horizontal plane 4. Adduction of the forefoot relative to the hindfoot in the horizontal plane Dimeglio A, Bensahel H, Souchet P, et al. Classification of clubfoot. J Pediatr Orthop B 1995;4:129–136.
- 45. Classificati on Grade Type Score Reducibility I Benign <5 > 90% soft-soft, resolving II Moderate 5 - <10 > 50% soft-stiff, reducible, partly resistant III Severe 10 - <15 < 50% stiff-soft, resistant, partly reducible IV Very Severe 15 - <20 < 10% stiff-stiff, resistant Dimeglio A, Bensahel H, Souchet P, et al. Classification of clubfoot. J Pediatr Orthop B 1995;4:129–136.
- 46. Composed of 10 different physical examination findings Each scored 0 for no abnormality, 0.5 for moderate abnormality, or 1 for severe abnormality. Each foot is assigned a total score, the maximum being 10 points, with a higher score indicating a more severe deformity
- 47. Pirani S. A reliable and valid method of assessing the amount of deformity in the congenital clubfoot. St. Louis, MO: Pediatric Orthopaedic Society of North America, 2004.
- 48. 1. Curvature of lateral border of foot 2. Severity of medial crease (foot held in maximal correction) 3. Severity of posterior crease (foot held in maximal correction) 4. Medial malleolar–navicular interval (foot held in maximal correction)
- 49. 1. Palpation of lateral part of head of talus (forefoot fully abducted) 2. Emptiness of heel (foot and ankle in maximal correction) 3. Fibula-Achilles interval (hip flexed, knee extended, foot and ankle maximally corrected)
- 50. 1. Rigidity of equinus (knee extended, ankle maximally corrected) 2. Rigidity of adductus (forefoot is fully abducted) 3. Long flexor contracture (foot and ankle held in maximal correction)
- 52. AP View: ◦ Talocalcaneal angle is reduced (normal 30-35°). It measures degree of varus. ◦ Talometatarsal angle is 0° to negative (normal 5- 15°). Indicates extent of forefoot adduction.
- 53. Lateral View: ◦ Talocalcaneal angle is reduced (normal 25-50°). It measures degree of varus. ◦ Tibiocalcaneal angle is negative in CTEV (normal 5-15°). Indicates extent of equinus.
- 54. Talocalcaneal Index: ◦ TC angle AP view + TC angle Lat view should be atleast 40°. It is reduced in CTEV.
- 55. • Conservative management • Surgical management • Management by external fixator
- 56. Soft tissue procedures are advocated for children <4years of age. For mild CTEV with no severe internal rotation deformity of calcaneus, a one-stage posteromedial release of TURCO is preferred.
- 57. For severe deformities a one-stage modified Mc-Kay procedure of both posteromedial and posterolateral release is preferred. Bony procedures are added to soft tissue procedures after 4years of age.
- 58. Done between 6-12months of age. Cincinnati’s incision is used. Structures released are: Medial: ◦ TP/AHL/FHL/FDL ◦ Capsules of ST/Tarsal/TM joints ◦ Ligaments-Deltoid/Plantar/Spring ligaments
- 59. Posterior: ◦ TA lengthening by z-plasty. ◦ Capsulotomy of ankle and subtalar joints. ◦ Calcaneofibular ligaments. Subtalar ligaments: ◦ Talocalcaneal ligaments ◦ Interosseous ligaments ◦ Bifurcated Y-ligaments.
- 60. Postoperative Regimen: ◦ Change cast at 2weeks. ◦ Long leg cast untill 3 months. ◦ Orthoses for 6-9 months.
- 61. Cincinnati’s incision. All structures on posteromedial side are released as in Turco. In addition, lateral structures released are: ◦ Suprior peroneal retinaculum ◦ Inferior external reticanulum ◦ Dorsal calcaneocuboid ligament ◦ Origin of extensor digitorum brevis.
- 62. Metatarsal osteotomy for metatarsus adductus. Dwyer’s lateral closing wedge osteotomy of calcaneus. Dillwyn Evan’s procedure: wedge resection from midtarsal area. Triple Arthrodesis.
- 63. Triple Arthrodesis: ◦ For children >10years. ◦ Functionally & cosmetically superior.Lateral closing wedge osteotomy through subtalar and midtarsal joints is done to fuse all three joints namely subtalar, talonavicular and calcaneocuboid. Talectomy: ◦ Used as a salvage procedure.
- 64. Garceaus Method: ◦ Transfer of tibialis anterior to middle cuneiform bone. Modified Garceaus Method: ◦ Transfer of tibialis anterior to base of 5th metatarsal.
- 65. Two types of frames: ◦ Ilizarov ◦ Joshi’s External Stabilization System (JESS) Semi-invasive, bloodless surgery and can be done without touraiquet. Technically demanding but avoids complications of surgery and scar. Corrects both bony and soft tissue component. If failure does occur, options of surgery are always open.