Recommended

Recommended
More Related Content
What's hot
What's hot (20)
Similar to PosterTemplate2010_Darowan_Aka_040510
Similar to PosterTemplate2010_Darowan_Aka_040510 (20)
PosterTemplate2010_Darowan_Aka_040510
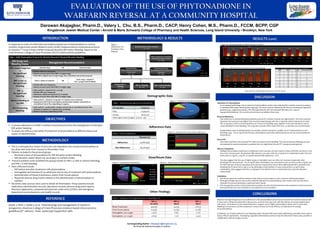
- 1. METHODOLOGY & RESULTS Darowan Akajagbor, Pharm.D., Valery L. Chu, B.S., Pharm.D., CACP, Henry Cohen, M.S., Pharm.D., FCCM, BCPP, CGP Kingsbrook Jewish Medical Center • Arnold & Marie Schwartz College of Pharmacy and Health Sciences, Long Island University • Brooklyn, New York Corresponding Author: Dakajagbor@kingsbrook.org No financial disclosures apply to authors INTRODUCTION In response to a lack of uniformity and evidence-based use of phytonadione to reverse warfarin, Kings brook Jewish Medical Center (KJMC) implemented an institutional protocol on January 1st 2009 to treat warfarin-induced elevated INR and/or bleeding based on the 2008 American College of Chest Physicians (ACCP) antithrombotic guidelines. OBJECTIVES To assess adherence to KJMC’s warfarin reversal protocol for the management of elevated INR and/or bleeding To assess the efficacy and safety of treatment of phytonadione at different doses and routes of administration METHODOLOGY This is a retrospective review of all acute care inpatients who received phytonadione at any dose and route from January to November 2009 Patients included in the protocol group: o Received a dose of phytonadione for INR elevation and/or bleeding o INR elevation and/or bleed was secondary to warfarin intake Protocol patients were stratified into groups based on INR ≥ 4 with or without bleeding, and INR ≤ 4 with bleeding Data collected include: o INR before and after treatment with phytonadione o Hemoglobin and hematocrit on admission and on day of treatment with phytonadione o Administration of blood transfusions and/or fresh frozen plasma o Reported adverse drug events related to the administration of phytonadione or warfarin Electronic data sources were used to obtain all information. These systems include medication administration records, laboratory records, adverse drug event reports, Pharmacy Application, computerized physician order entry (CPOE), and emergency department and ambulatory care health records. REFERENCE Ansell J, Hirsh J, Hylek E, et al. Pharmacology and management of vitamin K antagonists: American College of Chest Physicians evidence-based clinical practice guidelines (8th edition). Chest. 2008;133(6 Suppl):160S-198S. RESULTS (cont) DISCUSSION Indication for Phytonadione In an unexpected finding, only 50 percent of phytonadione orders were indicated for warfarin reversal secondary to elevated INRs and/or bleed (protocol group). The most common indications for the rest included pre-operative patients (e.g., surgical procedures, PEG tube placements) with non-elevated INR and a few cases of hypoprothrombinemia. The current protocol does not address these uses. Protocol Adherence Non-adherence to institutional phytonadione protocol for warfarin reversal was high (65.8%). The most common deviation from protocol was higher than recommended dosing, with the 10 mg dose used in nearly 60% of cases. The 10 mg dose, which is recommended as an IV dose for bleeding cases, appears to be only indicated in 34% of cases identified to have bleeding. The 5 mg dose was also often used where the 2.5 mg dose was recommended. Inappropriate route of administration was another common deviation, notably use of IV phytonadione in non- bleeding cases. The 10 mg PO and IM dose combinations were often administered but are not recommended by the protocol. Use of FFP One third of patients who received FFP were not found to have bleeding. This may be because bleeding was not documented in records evaluated or patients had very high bleed risk and FFP was given preemptively. Efficacy Comparison Multiple phytonadione dose/route combinations were used but all were noted to reduce INR after one dose. In the four most common pairs, the greatest INR reduction was seen with the 10 mg dose IV combination (74%). The next three pairs (10 mg PO, 5 mg PO, 10 mg IM) lowered INR similarly by ~ 50%. The data suggest that the use of higher doses or injectable route are often not necessary (especially when deviating from the protocol). The 10 mg PO dose combination was used almost twice as much as the 5 mg PO, but the INR reduction is almost equivalent (50% and 55% respectively), hence little additional benefit is obtained from doubling the PO dose from 5 mg to 1o mg. Although a small number of cases received the 2.5 mg PO dose combination, data suggests that the 2.5 mg dose is not inferior to the 10 mg SQ dose (54 % and 31% reduction respectively) Limitations We did not assess for warfarin resistance that may occur secondary to over-correction with phytonadione. Although multiple sources were used to identify indication for phytonadione, chart review was not done and a rationale for protocol deviations could have been missed. The retrospective nature of this review does not allow for the full clinical picture to be analyzed, so there may have been justification for uses classified as non-adherent in this evaluation. CONCLUSIONS Based on the high frequency of non-adherence to the phytonadione use protocol, the need to in-service medical staff is clear, but it will also be beneficial to discuss any concerns they may have with the efficacy of recommended doses and routes. No evidence in the medical literature supports use of higher phytonadione doses and IV route when bleeding is not present, and this evaluation’s review of dose and route efficacy corroborates the existing recommendations. In addition, use of phytonadione in non-bleeding and/or elevated INR cases needs addressing, especially when used to reduce INR pre-operatively. Developing a separate phytonadione protocol may be indicated in these cases, possibly in collaboration with the Surgery service. EVALUATION OF THE USE OF PHYTONADIONE IN WARFARIN REVERSAL AT A COMMUNITY HOSPITAL Table 1. KJMC Phytonadione Protocol for Warfarin Reversal in Elevated INR and/or Bleeding INR Range and Bleeding Status Management Recommendations INR >target range but <5 No significant bleeding ↓ Warfarin dose OR Omit next dose • Monitor INR more frequently • Resume at lower dose when INR is in target range • When INR is slightly above target range, dose reductions may not be necessary INR >5 but <9 No significant bleeding Omit 1-2 doses of warfarin OR Omit 1 dose + vitamin K P.O. 2.5 mg (if risk for bleed) • Monitor INR more frequently • Resume at lower dose when INR is in target range INR >9 No significant bleeding • Hold warfarin + vitamin K P.O. 2.5-5 mg • Monitor INR more frequently • Administer additional vitamin K P.O. if needed • Resume at lower dose when INR is in target range Serious bleeding at any INR • Hold warfarin + vitamin K 10 mg slow I.V. infusion over 30 minutes • Supplement with fresh frozen plasma, prothrombin complex concentrate, or recombinant Factor VIIa, depending on urgency Life-threatening bleeding • Hold warfarin + prothrombin complex concentrate or recombinant Factor VIIa + vitamin K 10 mg slow I.V. infusion over 30 minutes • Repeat if necessary, depending on INR Table 2. Protocol Group Age and Sex Distribution Demographic Frequency Male 55 (39.0%) Female 86 (61.0%) Mean Age in years (range): 75.3 (25 – 95) Table 3. Protocol Adherence Percent (n) Adherence 34.8% (49) Non-Adherence 65.2% (92) Other Findings Table 6. Mean INR Reduction By All Dose/Route Combinations DOSE ROUTE ↓ IN INR TOTAL PER GRP (n) 2.5 IV 6.78 1 2.5 PO 3.33 5 2.5 SQ 5.7 1 5 IM 3.07 2 5 IV 5.27 4 5 PO 2.91 34 7.5 PO 2.29 1 10 IM 2.62 12 10 IV 5.1 46 10 PO 3.88 20 10 SQ 1.53 4 Figure 1. Medication Use Evaluation Flow Diagram 65% 19% 16% INR > 4 INR >4 + Bleed INR < 4 + Bleed Figure 2. Protocol Group Distribution 6.5 8.5 9.02 9.3 0 2 4 6 8 10 PO IM IV SQ PO IM IV SQ Figure 6. Mean Doses for Different Routes of administration Figure 8. Mean Reduction in INR from Day 0 to Day 1 Mean dose Figure 9. INR Reduction By Most Common Dose/Route Combinations %INRreductionMeanINR All phytonadione orders reviewed (n = 526) Doses not given or subsequent doses given within 24-hours (n = 229) Non-Protocol Group Phytonadione for non-protocol indications (n = 148) Elevated INR ≥4 + Bleeding (n = 26) INR ≤4 + Bleeding (n = 22) INR ≥4 without Bleeding (n = 93) Protocol Group Phytonadione for elevated INR and/or bleed (n = 141) Mean time from phytonadione dose to day 1 INR (16.7 hours) Figure 5. Dose/Route Distribution 25% (36) 15% (21) 9% (13) 35% (49) 16% (22) 5 (PO) 10 (PO) 10 (IM) 10 (IV) OTHERS n = 141 OTHERS – 2.5 IV; 2.5 SQ; 2.5 PO; 5 IV; 5 IM; 7.5 PO; 10 SQ Figure 4. Reasons for Protocol Non-adherence 62.0% 81.5% 1.0% 0.0% 10.0% 20.0% 30.0% 40.0% 50.0% 60.0% 70.0% 80.0% 90.0% Incorrect route Dose (too high) Dose (too low) Figure 3 . Protocol Group Service Distribution 63% (89) 16% (22) 11% (15) 11% (15) Medicine ED Critical Care Rehab N = 141 31 50 50 54 55 74 0 10 20 30 40 50 60 70 80 10 mg 5 mg 10 mg 2.5 mg 10 mg 10 mg SQ PO IM PO PO IV Table 5. Frequency of Surrogate Markers for Bleeding % (n) INR ≥4 No bleed INR ≥4 Bleed INR <4 Bleed Blood Transfusion 9.9 (14) 3.5 (5) 7.8 (11) Fresh frozen plasma 6.4 (9) 6.3 (9) 5.7 (8) Hemoglobin ↓ by ≥4 g/dL 1.4 (2) 0 (0) <1 (1) Hemoglobin ↓ to <7 g/dL 2.8 (4) <1 (1) 1.4 (2) 9.5 6.18 7.37 8.76 6.77 5.86 5.31 5.2 6.88 7.06 4.94 2.72 2.85 1.67 5.7 1.51 2.96 2.29 2.58 1.78 3.18 3.41 0 2 4 6 8 10 2.5 mg 2.5 mg 2.5 mg 5 mg 5 mg 5 mg 7.5 mg 10 mg 10 mg 10 mg 10 mg IV PO SQ IM IV PO PO IM IV PO SQ DAY 0 INR DAY 1 INR Dose/Route Data Adherence Data Demographic Data