1. CAROLINE MOSESSIAN, PH.D., DRSC.,
FACMPE
REGULATORY SCIENCE PROGRAM
USC SCHOOL OF PHARMACY
DECEMBER 4, 2015
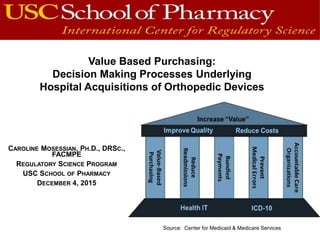
Value Based Purchasing:
Decision Making Processes Underlying
Hospital Acquisitions of Orthopedic Devices
Source: Center for Medicaid & Medicare Services
2. Background
Rising Healthcare costs have forced government, healthcare providers and
medical products companies to justify purchasing decisions.
Hip & Knee Implants are Expensive and Performed Frequently
Estimated increase of 174% for hip replacements and 673% for knee replacements
(Kurtz et al. 2007)
Medicare spending rising from $5 billion in 2006 to almost $50 billion in 2030
(Wilson et al. 2008)
Source: Center for Medicaid & Medicare Services
VBP: Strategy used by payers,
employers and federal government
to use market power as a force to
promote quality and value of
healthcare services.
3. Value Analysis Processes
&
Decision Making
Value-Based
Purchasing
Organization’s
Capabilities to
Evaluate
Alternatives &
Options
Data Integration
on Price, Quality
& Performance
Alignment of
Financial
Incentives &
Clinical Decision-
Making
4. Statement of the Problem
Fragmentation and Misalignment
• Strained Relationship between Physicians & Hospitals
• Physicians’ Strong Affinities with Device Firms
• Shifts of Surgical Facilities to Competing Sites
Misalignment of Incentives
• Dealing with Physicians Preference Items
• Financial Disclosure Policies for Physicians
• Battle over Gains-sharing Incentives
Organizational Coordination
• Hospital’s Capability to Acquire Innovative Technology (Medical Arm Race)
• Tighter Reimbursements from Payers
• Service Lines, Performance Measurements, Efficiency Ratios & Financial Accountability
Obstacles to VBP
5. Consumer Information Processing
Model
Retrieved fro: Matsuno(1997) http://faculty.babson.edu/isaacson/M_E7000/cons/cons1.doc
Problem Recognition
Information Search
Evaluation and Selection of Alternatives
Decision Implementation
Post-Purchase Evaluation
7. Delimitations
1
• United States Only
2
• Orthopedic Surgeons (Hip & Knee Specialists)
• Hospital Administrators
3
• Hip & Knee Implants Only
8. Limitations
1
• Biases of all Respondents
• Biases of the Investigator
2
• Type of Questions & Reported Data
3
• Challenges of Sample Size (Response Rate)
9. Methods
HOSPITAL &
HEALTH
SYSTEMS
• EXECUTIVES (CEO, CFO,
SERVICE LINES ETC.)
• SUPPLY CHAIN
MANAGEMENT/
PROCUREMENT OFFICER
ORTHOPEDIC
SURGEONS
• AFFILIATED WITH:
• HOSPITALS
• HEALTH SYSTEMS
• (ACADEMIC/COMMUNITY
ETC.)
10. Methods (cont’d)
On-line survey instrument using Qualtrics
Focus group critiqued the survey and assessed content
validity
• Approximately 26 questions
• Combination of “Yes/No”, Choose One, Scaled and Open
Ended
Survey target population was accessed by:
• Direct Technique
• Snowball Technique (Members of AAOS, Executive and
Orthopedic colleagues to forward survey)
11. 26 (38%) affiliated with
academic health system
20 (29%) part of independent
health system
16 (23%) community or
specialty hospital
5 (7%) with HMO (e.g.,
Kaiser Permanente)
10 (14%) affiliated with
public/state & Other facilities
Other
GPO/Purchasing consultants
Hospital Purchasing Director
Hospital Director
Orthopedic Surgeon
(40 or 58%)
69 individuals responded (36% response rate) based on 193 surveys deployed
Profile of Respondents
(29 or 42%)
Majority (33 or 48%)
were part of a
medium-sized
facility (200-450
beds)
Locations
throughout
USA, (42 or
60%) from
Westcoast
12. Average of 7 Orthopedic (hip and
knee) surgeons practiced in the
facilities
4 was the mean # of orthopedic hip
and knee implants used in the
facilities
Profile of Respondents
13. Institutional structures in decision-making:
39 (57%) by orthopedic surgeons
38 (55%) Committee (e.g., VAC, P&T etc.)
15 (22%) separate committee for orthopedic products only
10 (19%) hospital administrators/executives made decisions
7 (10%) other (e.g., health system has negotiated pricing)
Structures & Data Gathering to base
Decision-Making
“Ask” & “Acquire”
14. Primary mechanism for decision-making for orthopedic implants:
26 (38%) by orthopedic surgeons (physician preference)
26 (38%) Committee (e.g., VAC, P&T etc.)
8 (12%) hospital administrators/executives made decisions
7 (10%) other (e.g., health system has negotiated pricing)
Structures & Data Gathering to base
Decision-Making
“Ask” & “Acquire”
15. Initiating person or group to purchase equipment:
55 (80%) by physicians
12 (17%) hospital administrators/directors
5 ( 7%) formal committee
5 ( 7%) other (e.g., health system or ortho. department or industry
reps)
Structures & Data Gathering to base
Decision-Making
“Ask” & “Acquire”
16. Evaluation and Selection of Devices
“Appraise & Aggregate”
Meeting frequency and committee membership/representation:
20 (38%) Monthly meetings VS 13 (25%) ad-hoc
One physician and one hospital administrator as members
Respondents were generally satisfied with committee membership
(between 7-10 members)
Decision Evaluation:
37 (54%) continuously evaluated reimbursement trends & device costs
35 (51%) continuously evaluated clinical outcomes
27 (39%) reconsidered the choice when utilization or volume dropped
12 (17%) believed no review of choices were made
Decision on novel, custom, or “compassionate use” devices:
36 (52%) same decision-making for regular equipment purchasing
19 (28%) special process (e.g., case-by-case, IRB approval/or CMO)
19 (28%) do not handle such cases
17. Making the Decision
“Apply”
Factors influencing purchasing decision-making:
60 (87%) physicians’ preferences
60 (87%) financial information (Reimbursement, ROI, expenses, etc.)
45 (65%) clinical outcomes
26 (38%) influencers (e.g., payers, sales rep, government policies)
10 (14%) patient preference
Importance of information/data in decision-making:
36 (52%) quality outcome data “RANKED AS HIGHEST”
33 (48%) manufacturer’s information “RANKED AS LOWEST”
29 (43%) believed that ad-hoc decisions are made
24 (36%) used numeric or ranking system to make decisions
18. Analysis of Survey Results
“Assess”
Assessment of validity of purchasing decisions:
33 (48%) re-evaluated when contracts were due for renewal
17 (24%) continuously evaluated their decisions
5 (7%) evaluated - problem with patient, product or payer
6 (9%) never evaluated
General views and satisfaction level on decision-making
processes/policies:
30 (43%) views of stakeholders are hard to align
38 (55%) hospital administration approves the implant purchase
37 (54%) affirmed that physicians maintain financial relationship (RWI)
46 (67%) were satisfied with the overall process
19. Summary
Some form of formalized decision-making exists
in healthcare systems
Still in evolution with foreseeable stresses during
the evolution
The pressure to save cost and increase
productivity is increasing
Creation of a US/HTA as US migrates to a
“single-payer” system
20. Future Evolution
Trend will continue due to governmental efforts to promote cost
containment.
CMS to have 30% of Medicare payments under “bundled contracts” by 2016
20 major health systems & health plans to have 75% of contracts under
“valued-based” incentives by 2020
Orthopedic implants will continue to be an important target for
cost containment initiatives nationally
CMS issued proposed rule July 2015 and finalized Nov. 16, 2015
the “episodic-based” payment for “CCJR” model (savings of over $150m ~ 5
years)
Changes in procedures and changes in roles (balance of power)