Gh foi combinado outras substâncias para potencializar impacto sobre estatura infantil,juvenil.
•Als DOCX, PDF herunterladen•
1 gefällt mir•637 views

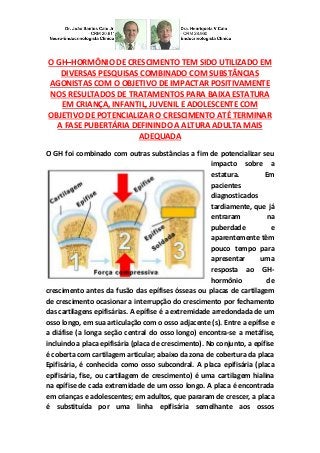
No conjunto, a epífise é coberta com cartilagem articular; abaixo da zona de cobertura da placa Epifisária, é conhecida como osso subcondral. A placa epifisária (placa epifisária, fise, ou cartilagem de crescimento) é uma cartilagem hialina na epífise de cada extremidade de um osso longo. A placa é encontrada em crianças e adolescentes; em adultos, que pararam de crescer, a placa é substituída por uma linha epifisária semelhante aos ossos consolidados.

Empfohlen
Weitere ähnliche Inhalte
Mehr von Van Der Häägen Brazil
Mehr von Van Der Häägen Brazil (20)
Kürzlich hochgeladen
Kürzlich hochgeladen (9)
Gh foi combinado outras substâncias para potencializar impacto sobre estatura infantil,juvenil.
- 1. O GH–HORMÔNIO DE CRESCIMENTO TEM SIDO UTILIZADO EM DIVERSAS PESQUISAS COMBINADO COM SUBSTÂNCIAS AGONISTAS COM O OBJETIVO DE IMPACTAR POSITIVAMENTE NOS RESULTADOS DE TRATAMENTOS PARA BAIXA ESTATURA EM CRIANÇA, INFANTIL, JUVENIL E ADOLESCENTE COM OBJETIVO DE POTENCIALIZAR O CRESCIMENTO ATÉ TERMINAR A FASE PUBERTÁRIA DEFININDO A ALTURA ADULTA MAIS ADEQUADA O GH foi combinado com outras substâncias a fim de potencializar seu impacto sobre a estatura. Em pacientes diagnosticados tardiamente, que já entraram na puberdade e aparentemente têm pouco tempo para apresentar uma resposta ao GH- hormônio de crescimento antes da fusão das epífises ósseas ou placas de cartilagem de crescimento ocasionar a interrupção do crescimento por fechamento das cartilagens epifisárias. A epífise é a extremidade arredondada de um osso longo, em sua articulação com o osso adjacente (s). Entre a epífise e a diáfise (a longa seção central do osso longo) encontra-se a metáfise, incluindo a placa epifisária (placa de crescimento). No conjunto, a epífise é coberta com cartilagem articular; abaixo da zona de cobertura da placa Epifisária, é conhecida como osso subcondral. A placa epifisária (placa epifisária, fise, ou cartilagem de crescimento) é uma cartilagem hialina na epífise de cada extremidade de um osso longo. A placa é encontrada em crianças e adolescentes; em adultos, que pararam de crescer, a placa é substituída por uma linha epifisária semelhante aos ossos
- 2. consolidados. A ossificação endocondral é responsável pelo desenvolvimento inicial do osso a partir da cartilagem no útero, de lactentes e do crescimento longitudinal dos ossos longos na placa epifisária. Na placa os condrócitos estão em constante divisão por mitose. Estas células filhas estão voltadas para a epífise, enquanto as células mais velhas são empurradas para a diáfise. Como os condrócitos mais velhos degeneram, os osteoblastos ossificam os restos para formar um novo osso. Na puberdade o aumento dos níveis de estrogênio, no gênero masculino e feminino, leva a um aumento da apoptose de condrócitos na placa epifisária. A depleção de condrócitos devido a apoptose provoca uma diminuição da ossificação e o crescimento abranda e depois pára, quando todas as cartilagens se tornaram ossos por substituição, deixando apenas uma cicatriz epifisária fina que depois desaparece. Uma vez que a fase adulta é atingida, a única maneira de manipular a altura ou estatura longitudinal ou linear é modificando o comprimento do osso através de distração osteogênica. Mas diversas pesquisas clínicas tem demonstrado que tem sido usado, a fim de retardar a fusão das epífises, um agonista do GnRH em estudos clínicos com variados índices de sucesso, além de substâncias como inibidores da Aromatase que promovem um ganho de um tempo maior com o retardo da puberdade e dificulta o fechamento da cartilagem de crescimento ou placa epifisária ou placa de crescimento, entretanto, além da experiência profissional na manipulação desta terapêutica relativamente nova, temos que ter a consciência que terminada a
- 3. puberdade, as terapias fisiológicas são aceitáveis como ajuda, as demais são agressivas e desaconselhadas para pessoas que já passaram por todas as fases e suas cartilagens de crescimento estão consolidadas por serem adultas, o que reforça o início precoce de qualquer terapêutica sendo aconselhada para que ocorra como primeira opção e este fato está ganhando espaço no meio científico e serve de orientação profissional. GH HAS BEEN COMBINED WITH OTHER SUBSTANCES FOR ITS POSITIVELY IMPACT ON HEIGHT LEVERAGE IN CHILD AND YOUTH. GH-GROWTH HORMONE HAS BEEN USED IN COMBINATION WITH SEVERAL POLLS AGONISTS SUBSTANCES IN ORDER TO POSITIVELY IMPACT ON RESULTS OF TREATMENT FOR LOW HEIGHT IN CHILD, INFANT, YOUTH AND TEEN WITH GOAL TO COMPLETE PHASE AND POTENTIATE PUBERTY SETTING THE STAGE ADULT MORE ADEQUATE: PHYSIOLOGY-ENDOCRINOLOGY-NEUROENDOCRINOLOGY-GENETICS- ENDOCRINE- PEDIATRICS (SUBDIVISION OF ENDOCRINOLOGY): DR. JOÃO SANTOS CAIO JR. ET DRA. HENRIQUETA VERLANGIERI CAIO. GH was combined with other substances in order to maximize its impact on the stature. In patients diagnosed late, which has already entered puberty and apparently have little time to submit a response to GH-growth hormone
- 4. before the fusion of the epiphyseal bone or cartilage growth plates lead to cessation of growth by closure of epiphyseal cartilage. The epiphysis is rounded end of a long bone in its articulation with the adjacent bone (s). Between the epiphysis and diaphysis (the long central section of the long bone) lies the metaphysis, including the epiphyseal plate (growth plate). Overall, the epiphysis is covered with articular cartilage; below which is a coverage area of the growth plate known as the subchondral bone. The epiphyseal plate (growth plate or, physis, or growth cartilage) is a hyaline cartilage plate at each end of the metaphysis of a long bone. The plate is found in children and adolescents; in adults who have stopped growing, the plate is replaced by a consolidated similar to bone epiphyseal line. Endochondral ossification is responsible for the initial development of bone from cartilage in the uterus and infants and the longitudinal long bone growth in the growth plate. The plate chondrocytes are under constant division by mitosis. These daughters cells toward the epiphysis, while older cells are pushed to the shaft. As the older chondrocytes degenerate, osteoblasts ossify the remains to form new bone. At puberty the increased levels of estrogen in males and females, leads to increased apoptosis of chondrocytes in the epiphyseal plate. The depletion due to apoptosis of chondrocytes causes a decrease in ossification and growth slows and then stops, when all of became cartilage replacement by bone, leaving only a thin epiphyseal scar then disappears. Once the adult stage is reached, the only way to manipulate the height or longitudinal linear or modifying the height and length of the bone is by distraction osteogenesis. However various clinical studies have demonstrated that has been used in order to delay the fusion of the epiphyses a GnRH agonist in clinical trials with varying success rates, as well as substances such as aromatase
- 5. inhibitors that provide a higher gain with time delayed puberty and impair closure of growth plates or epiphyseal plate or growth plate, however besides professional experience in handling this relatively new therapy, we have to be aware that finished puberty, physiological therapies are acceptable as aid, others are aggressive and discouraged for people who have gone through all stages and are consolidated their growth cartilage by being adult, which reinforces early initiation of any therapy being advised that occurs as a first option and this fact is gaining ground in scientific means serves the professional guidance. Dr. João Santos Caio Jr. Endocrinologia – Neuroendocrinologista CRM 20611 Dra. Henriqueta V. Caio Endocrinologista – Medicina Interna CRM 28930 Como saber mais: 1. Foram estudados 52 pacientes (muitos desde o nascimento) durante toda a infância, puberdade e na idade adulta. Foi descoberto que os recém-nascidos com deficiência de IGF-I (LS) são ligeiramente mais curtos no nascimento medindo em torno de 42 a 47 cm do que os bebês saudáveis que mediam em torno de 49 a 52 cm, sugerindo que o IGF-I tem alguma influência sobre o crescimento linear intrauterino... http://hormoniocrescimentoadultos.blogspot.com 2. Este fato é reforçado pelos resultados que já no momento do nascimento, e durante toda a infância, a maturação esquelética é retardada, assim como é o crescimento dos órgãos... http://longevidadefutura.blogspot.com 3. A deficiência de IGF-I também provoca o subdesenvolvimento e a fragilidade do sistema muscular e prejudica e enfraquece o cabelo e o crescimento das unhas...
- 6. http://imcobesidade.blogspot.com AUTORIZADO O USO DOS DIREITOS AUTORAIS COM CITAÇÃO DOS AUTORES PROSPECTIVOS ET REFERÊNCIA BIBLIOGRÁFICA. Referências Bibliográficas: Caio Jr, João Santos, Dr.; Endocrinologista, Neuroendocrinologista, Caio,H. V., Dra. Endocrinologista, Medicina Interna – Van Der Häägen Brazil, São Paulo, Brasil; Allen JP, Land D. Attachment in adolescence. In: Cassidy J, Shaver PR, editors. Handbook of attachment: Theory, research, and clinical applications. New York: Guilford; 1999. pp. 319–335; BeLue R, Francis LA, Colaco B. Mental health problems and overweight in a nationally representative sample of adolescents: Effects of race and ethnicity. Pediatrics. 2009; 123 :697–702. doi: 10.1542/peds.2008-0687; Bolton-Smith C, Woodward M, Tunnstall-Pedoe H, Morrison C. Accuracy of the estimated prevalence of obesity from self reported height and weight in an adult Scottish population. Journal of Epidemiology and Community Health. 2002; 54 :143–148; Brener ND, McManus T, Galuska DA, Lowry R, Wechsler H. Reliability and validity of self-reported height and weight among high school students. Journal of Adolescent Health. 2003; 32 :281–287. doi: 10.1016/S1054-139X(02)00708-5; Caruthers AS, Van Ryzin MJ, Dishion TJ. Preventing high risk sexual behavior in early adulthood with family interventions in adolescence. Prevention Science (in press); Collins L, Murphy S, Bierman K. A conceptual framework for adaptive preventive interventions.Prevention Science. 2004; 5 :185–196. doi: 10.1023/B:PREV.0000037641.26017.00; Connell A, Dishion TJ. Reducing depression among at-risk early adolescents: Three-year effects of a family-centered intervention embedded within schools. Journal of Family Psychology. 2008; 22 :574– 585. doi: 10.1037/0893-3200.22.3.574; Danielsson P, Svensson V, Kowalski J, Nyberg G, Ekblom O, Marcus C. Importance of age for 3-year continuous behavioral obesity treatment success and dropout rate. Obesity Facts. 2012; 5 :34–44. doi: 10.1159/000336060; Davis M, Gance-Cleveland B, Hassink S, Johnson R, Paradis G, Resnicow K. Recommendations for prevention of childhood obesity. Pediatrics. 2007; 120 :S229–S253; Davison KK, Birch LL. Childhood overweight: A contextual model and recommendations for future research. Obesity Reviews. 2001; 2 :159–171. Contato: Fones: 55 11 5087-4404 ou 96197-0305 Nextel: ID:111*101625 Rua Estela, 515 - Bloco D - 12º andar - Conj. 121/122 Paraiso - São Paulo - SP - Cep 04011-002 e-mails: drcaio@vanderhaagenbrasil.com drahenriqueta@vanderhaagenbrasil.com vanderhaagen@vanderhaagenbrasil.com Site Van Der Häägen Brazil www.vanderhaagenbrazil.com.br www.clinicavanderhaagen.com.br
- 7. www.crescimentoinfoco.com www.obesidadeinfoco.com.br http://drcaiojr.site.med.br http://dracaio.site.med.br Joao Santos Caio Jr http://google.com/+JoaoSantosCaioJr Video http://youtu.be/woonaiFJQwY Google Maps: http://maps.google.com.br/maps/place?cid=5099901339000351730&q=Van+Der+Haagen+Brasil&hl= pt&sll=-23.578256,46.645653&sspn=0.005074,0.009645&ie =UTF8&ll=-23.575591,- 46.650481&spn=0,0&t = h&z=17