
Empfohlen
Weitere ähnliche Inhalte
Was ist angesagt?
Was ist angesagt? (20)
Ähnlich wie 4 macrocytic anemia.ppt
Ähnlich wie 4 macrocytic anemia.ppt (20)
Mehr von AbdulKaderSouid
Mehr von AbdulKaderSouid (14)
Kürzlich hochgeladen
Kürzlich hochgeladen (20)
4 macrocytic anemia.ppt
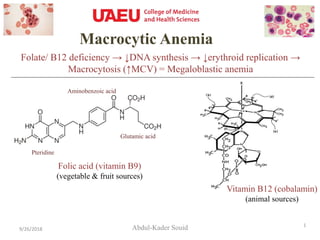
- 1. Macrocytic Anemia Abdul-Kader Souid9/26/2018 1 Folate/ B12 deficiency → ↓DNA synthesis → ↓erythroid replication → Macrocytosis (↑MCV) = Megaloblastic anemia Vitamin B12 (cobalamin) (animal sources) Folic acid (vitamin B9) (vegetable & fruit sources) Pteridine Aminobenzoic acid Glutamic acid
- 2. Megaloblastic Anemia • The cause is usually a deficiency of folate or vitamin B12 (cobalamin). It produces distinctive erythroid and neutrophil morphologic abnormalities. 9/26/2018 2 In megaloblastic anemia, the marrow is cellular; the anemia results from ineffective erythropoiesis (active erythropoiesis with ↓red cell production). Normal marrow Megaloblastic marrow Hypersegmented neutrophils Must know
- 3. Folate (Vitamin B9) Sources • Vegetables: Asparagus, broccoli, spinach, lettuce, beans • Fruits: Oranges, lemons, bananas, strawberries, melons • Others: Liver, kidney, mushrooms, peanuts – Folate is depleted by excessive cooking. 9/26/2018 Deficiency • Malabsorption: Gluten-induced enteropathy (celiac disease), Crohn disease, gastrectomy, jejunal resection, poor nutrition, alcoholism. ↑Requirement • Pregnancy & infancy (rapidly proliferating tissues) • Hemolytic anemia (folate is not reutilized after performing its coenzyme functions). Must know
- 4. Folate Deficiency → Neural Tube Defects Folate supplement (0.4 mg daily) before conception and in the first 12 weeks of pregnancy reduces the incidence of neural tube defects (spina bifida) in the fetus by about 50%. The incidence of cleft palate is also reduced. 9/26/2018 4 ↓Folate → ↓Pyrimidine & Purine Synthesis → ↓Cell Replication Must know Meningomyelocele Cleft palateCleft lip
- 5. Folate-mediated Methylation (CH3) Reactions 5,10-methylene-tetrahydrofolate dUMP dTMP A B Must know ↓Folate → ↓dTMP (↓pyrimidine synthesis) + ↓Conversion of homocysteine to methionine (↑thrombophilia, ↑ischemic heart disease & ↑stroke) Important: 5,10-methylene-tetrahydrofolate (5,10-CH2-THF) is needed for converting dUMP (deoxyuridine monophosphate) to dTMP (deoxythymidine monophosphate). 5,10-CH2-THF is decreased in cobalamin/ folate deficiency.
- 6. Homozygous C677T in the methylene tetrahydrofolate reductase (MTHFR) gene → ↓Activity of MTHFR → ↑homocysteine → ↑thrombophilia + ↑ischemic heart disease + ↑stroke 6 MTHFR = Methylene Tetrahydrofolate Reductase THF = Tetrahydrofolate MTHFR Optional ↑Homocysteine is thrombogenic.
- 7. Vitamin B12 (Cobalamin) = Cobalt atom at center of corrin ring Sources • Animal sources only: Shellfish, liver, fish, crustaceans (crab), red meat, dairy products, eggs – Vegetables, fruits, and foods of non-animal origin are free from cobalamin. 7 Deficiency (Human stores sufficient cobalamin for 3 years.) • Nutritional → Vegans • ↓Intrinsic factor (IF) → Pernicious anemia, gastrectomy • Malabsorption → Ileal resection, Crohn disease, stagnant (blind) loop • Transcobalamin deficiency (detected by newborn screening) B12 Must know
- 8. • Cobalamin is absorbed in the ileum, mediated by the gastric intrinsic factor (IF). • IF is produced in the gastric parietal cells; its secretion parallels that of hydrochloric acid (HCl). • The IF-cobalamin complex enters the ileal cell, where IF is destroyed. • Cobalamin appears in portal blood attached to transcobalamin-II (TC-II) and delivered to the liver, bone marrow and other tissues. 8 Cobalamin (Vitamin B12) Must know Cobalamin is responsible for critical metabolic pathways, including folate-mediated reactions and folate recycling.
- 9. Cobalamin Exists in Two Biologic Forms (1) Methylcobalamin → in the cytosol → cofactor for methionine synthase: (homocysteine → methionine) (2) Adenosylcobalamin (AdoCbI) → in the mitochondria → cofactor for methylmalonyl coenzyme A (CoA) mutase: (methylmalonyl CoA → succinyl CoA) - an intermediate of the citric acid cycle Must know
- 10. Neurologic Manifestations: • Cobalamin deficiency causes peripheral neuropathy, demyelination of the pyramidal tracts of the spinal cord and optic atrophy. • Patients present with paresthesia, weakness, difficulty in walking, dementia, psychotic disturbances, and visual impairment. • Long-term nutritional cobalamin deficiency in infancy leads to poor brain development and impaired intellectual development. 10 Cobalamin Deficiency Scherer K. Images in clinical medicine. Neurologic manifestations of vitamin B12 deficiency. N Engl J Med. 2003 May 29;348(22):2208. “A 56-year-old woman presented with a four-month history of progressive cognitive decline, weakness, incoordination, and gait disturbance. She had severe ataxia; reflexes, vibratory sensation, and the sense of position were absent. Brain MRI demonstrated extensive areas of high-intensity signal in the periventricular white matter. Spine MRI showed a hyperintense signal along the posterior columns in all segments. Laboratory tests revealed macrocytic anemia, hypersegmented neutrophils, a low serum vitamin B 12 (34 pg per milliliter [25 pmol per liter]), and anti–intrinsic-factor antibodies (pernicious anemia). Vitamin B12 injections rapidly improved cognitive function, strength and walking.” Optional
- 11. Pernicious Anemia • The term pernicious anemia is reserved for ↓secretion of intrinsic factor (IF) by atrophic gastric mucosa. It has insidious onset that begins after 40 y of age. • It results from immune destruction of the acid- and pepsin-secreting gastric parietal cells (achlorhydria), causing atrophic gastritis and reduced intrinsic factor (IF) secretion. Achlorhydria increases the risk of gastric cancer. • Studies suggest the gastric atrophy in pernicious anemia is caused by CD4+ T-cells whose receptors recognize the H+/K+-ATPase (i.e., autoimmune disease). • Antibodies to intrinsic factor (type I, "blocking" antibodies) or the intrinsic factor–cobalamin complex (type II, "binding," antibodies) are highly specific to pernicious anemia. Must know Gastric Mucosa • Other autoimmune diseases (e.g., thyroiditis, type 1 diabetes, celiac disease, and Addison disease) frequently exist. • Measurement of anti-intrinsic factor (IF) antibodies in serum confirms the diagnosis of pernicious anemia.
- 12. DIAGNOSIS OF COBALAMIN & FOLATE DEFICIENCIES • ↓ Serum Cobalamin • Serum cobalamin is measured by an enzyme-linked immunosorbent assay (ELISA). Normal levels are ≥148 pmol/L (200 ng/L). Patients with megaloblastic anemia have levels <74 pmol/L (100 ng/L). Values of 74-148 pmol/L (100-200 ng/L) are borderline. • ↑ Serum methylmalonate and homocysteine • ↑ Intrinsic Factor (IF) & Parietal Cell Antibodies (=pernicious anemia) • ↓ Serum Folate: Normal = 11-82 nmol/L (2-15 µg/L). Serum folate reflects recent diet. • ↓ Red Cell Folate • It is less affected by recent diet and sample hemolysis • Normal values are 880–3520 µmol/L (160–640 µg/L) of packed red cells. 12 Must know
- 13. High-doses of oral vitamin B12 can be used to treat patients with megaloblastic anemia, including those with pernicious anemia. Which one of the following statements about oral vitamin B12 administration to patients with megaloblastic anemia and pernicious anemia is correct? A. It is effective only in patients with normal intrinsic factor secretion. B. It is not effective in patients with anti-intrinsic factor antibodies. C. It is not effective in patients with atrophic gastritis. D. Its dose is the same as parenteral vitamin B12. E. Treatment requires close monitoring to assure compliance. F. Methylmalonate and homocysteine levels increase with the treatment. 9/26/2018 13
- 14. 1. Pernicious anemia 2. Megaloblastic anemia 3. ↑MCV 4. Ineffective erythropoiesis 5. Neural tube defects 6. ↑Cardiovascular disease 7. Neurological manifestations 8. ↑Serum methylmalonate 9. Animal sources 10. ↓DNA synthesis 11. Achlorhydria 12. Intrinsic factor (IF) antibody 9/26/2018 14 A. Folate B. Cobalamin C. Both
- 15. Required Reading 1. Williams Hematology – Chapter 41. Folate, Cobalamin, and Megaloblastic Anemias 2. Harrison’s Online – Chapter 105. Megaloblastic Anemias 3. Stabler SP. Clinical practice. Vitamin B12 deficiency. N Engl J Med. 2013;368:149-60. 4. Heilman CB, Zerris VA. Images in clinical medicine. Combined-system disease. N Engl J Med. 2009;360:2655. 5. Balcı YI, Ergin A, Karabulut A, et al. Serum vitamin B12 and folate concentrations and the effect of the Mediterranean diet on vulnerable populations. Pediatr Hematol Oncol 2014;31:62. 9/26/2018 15