Case record...Arterial ectasia of the vertebro-basilar system
•
0 gefällt mir•1,842 views

Case record...Arterial ectasia of the vertebro-basilar system

Weitere ähnliche Inhalte
Was ist angesagt?
Was ist angesagt? (20)
Ähnlich wie Case record...Arterial ectasia of the vertebro-basilar system
Ähnlich wie Case record...Arterial ectasia of the vertebro-basilar system (20)
Mehr von Professor Yasser Metwally
Mehr von Professor Yasser Metwally (20)
Kürzlich hochgeladen
Kürzlich hochgeladen (20)
Case record...Arterial ectasia of the vertebro-basilar system
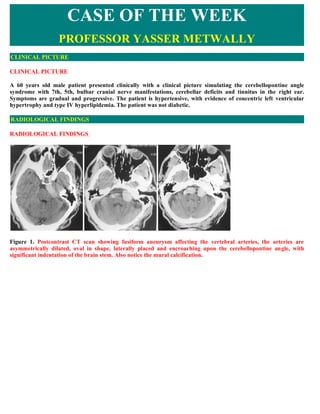
- 1. CASE OF THE WEEK PROFESSOR YASSER METWALLY CLINICAL PICTURE CLINICAL PICTURE A 60 years old male patient presented clinically with a clinical picture simulating the cerebellopontine angle syndrome with 7th, 5th, bulbar cranial nerve manifestations, cerebellar deficits and tinnitus in the right ear. Symptoms are gradual and progressive. The patient is hypertensive, with evidence of concentric left ventricular hypertrophy and type IV hyperlipidemia. The patient was not diabetic. RADIOLOGICAL FINDINGS RADIOLOGICAL FINDINGS Figure 1. Postcontrast CT scan showing fusiform aneurysm affecting the vertebral arteries, the arteries are asymmetrically dilated, oval in shape, laterally placed and encroaching upon the cerebellopontine angle, with significant indentation of the brain stem. Also notice the mural calcification.
- 2. Figure 2. Postcontrast scan showing fusiform aneurysm affecting the vertebral arteries, the arteries are asymmetrically dilated, oval in shape, laterally placed and encroaching upon the cerebellopontine angle, with significant indentation of the brain stem. Also notice the mural calcification. Figure 3. Precontrast CT scans showing basilar artery fusiform aneurysm, notice the rounded configuration, the midline location in the prepontine cistern, and the precontrast hyperdensity that could be due to thrombosis ( density below that of calcification). Figure 4. Conventional angiography showing basilar artery fusiform aneurysm. Mural thrombosis is probably present.
- 3. DIAGNOSIS: DIAGNOSIS: FUSIFORM ANEURYSM OF THE VERTEBROBASILAR SYSTEM WITH MURAL THROMBOSIS DISCUSSION DISCUSSION Fusiform aneurysms are enlarged, elongated and tortuous arterial segments. They are characterized by a lengthy course, lack of a defined neck and by the circumferential involvement of the parent vessels, Schnee and Flamm, 1997. Fusiform aneurysms represent a spectrum of non saccular, diffuse, segmental dilatation of the affected artery rather than focal, berry dilatation seen in saccular aneurysms, Mizutani and Aruga, 1992, Gobin et al, 1996, Perforating vessels often arises from the dome of the dilated vessels. Anson et al, 1996 Sustained arterial hypertension results initially in vascular smooth muscle cell proliferation that ultimately ends in loss of muscle fibre and its replacement by elastic, collagen and fibrous tissues. The internal elastic lamina fragments, splits and degenerate resulting either in diffuse concentric stenosis or diffuse dilatation (ectasia) of the artery (fusiform aneurysms). This pathology is either static or slowly progressive. Stenosis never results in complete occlusion or distal embolization, its significance is in the continuing narrowing with resultant of reduction of blood flow. The vertebro-basilar system is more frequently involved in hypertension resulting in either arterial stenosis or dilatation (ectasia) with frequent elongation and tortuosity of the arteries. Weir, 1987, Mizutani and Aruga, 1992, Metwally 2001, Metwally and Refaat, 1999, Gobin et al, 1996, Schnee and Flamm, 1997, Metwally, 2008 Pathological findings, in fusiform aneurysms, include absence of the intima, extensive fibrosis and deficiencies of the muscularis and internal elastic lamina and irregular thickening of the media, Schnee and Flamm, 1997. Berry (saccular) aneurysms differ from fusiform aneurysms in that saccular aneurysms arise from congenital, acquired, or iatrogenic medial defects with or without atherosclerosis, and hypertension or develop after intima disruption from dissection. Weir, 1987, Mizutani and Aruga, 1992, Gobin et al, 1996, Schnee and Flamm, 1997, Metwally 2001, Metwally, 2008 Unlike fusiform aneurysms, berry (saccular) aneurysms are focal dilatations that occur at the point of arterial bifurcations with a definite neck, Mizutani and Aruga, 1992, Gobin et al, 1996, Schnee and Flamm, 1997. Circumferential intraluminal laminated thrombosis is common in fusiform aneurysms and causes ischemia by directly impairing blood flow, by obscuring the origin of the perforating vessels or by embolization, Schnee and Flamm, 1997. Fusiform aneurysms rarely rupture of cause subarachnoid haemorrhage, Weir, 1987, Mizutani and Aruga, 1992, Gobin et al, 1996, Schnee and Flamm, 1997. Fusiform aneurysms may attain a huge size and induce significant compression of the nearby neural structures, Redekop and Ferguson, 1995. These aneurysms are occasionally asymptomatic and represent an incidental CT scan or MRI findings. Gobin et al, 1996, Schnee and Flamm, 1997, Metwally, 2008 In the study of Metwally, 2001 of 9 cases with fusiform aneurysm, hypertension was the main risk factor for the development of fusiform aneurysms, since it was universally present in all patients included in the study. Left ventricular hypertrophy could be regarded as a marker of increased susceptibility for the development of these aneurysms since it it was also present in all patients in the study of Metwally, 2001. The role of diabetes as a risk factor for the development of these aneurysms is questionable since it was present in only one patient in the sudy of Metwally, 2001. The male preponderance reported in this study was not touched in any of the reviewed literature. Metwally 2001, Metwally, 2008 Subarachnoid haemorrhage is a rare occurrence in fusiform aneurysm patients Fusiform aneurysms (unlike saccular aneurysms) rarely rupture or produce subarachnoid haemorrhage (unless associated with berry aneurysms) but rather they symptomatize by inducing ischaemic manifestations or by compression of neural structures. Schnee and Flamm, 1997 Gobin et al, 1996, Schnee and Flamm, 1997, Metwally 2001, Metwally, 2008 Brain parenchymal involvement is not uncommonly associated with fusiform aneurysm. In the study of Metwally, 2000 of 9 patients with fusiform aneurysm, patients with parenchymal involvement were divided into three groups.
- 4. Those with ischemic or haemorrhagic parenchymal changes that are probably not causally related to the existing fusiform aneurysms (33%), those with ischemic parenchymal changes that could be causally related to the existing fusiform aneurysms (33%) and patients without any parenchymal brain changes other than brain stem indentation by the aneuryms, Metwally, 2001,2008 Table 1. The clinical picture and result of brain imaging in Metwally 2001 patients with fusiform aneuryms Metwally, 2001, 2008 Number age Clinical picture Brain parenchymal abnormalities 1 75 Clinical picture of multi-infarct Multiple lacunar infarctions, leukoaraiosis, Central dementia due to multiple lacunar and cortical atrophy (CT scan) infarctions 2 64 Locked-in syndrome due to midbrain Massive pontine-midbrain infarction (CT scan) infarction 3 66 Stroke due to left putameno-capsular Left putameno-capsular hypertensive haematoma hypertensive haematoma 4 78 Left hemiplegia due to pontine Pontine infarction (MRI) infarction 5 70 Right hemiplegia due to left capsular Left capsular lacunar infarction (CT scan) lacunar infarction 6 68 Left hemiplegia due to pontine Pontine infarction (MRI) infarction 7 54 Multiple cranial nerve palsies, attacks of No parenchymal abnormalities other than brain stem vertigo, vascular headache, long tract indentation by the aneuryms (MRI, CT scan) manifestations. 8 51 Multiple cranial nerve palsies, long tract No parenchymal abnormalities other than brain stem manifestations. indentation by the aneuryms (MRI, CT scan) 9 57 Migraine resistant to treatment No parenchymal abnormalities (MRI, CT scan) Table 2. Patients with parenchymal involvement are classified into three groups as follows Metwally, 2001, 2008 No. Description Number of patients % 1 With cerebral lesions 3 33 % 2 With brain stem ischemic 3 33 % lesions 3 No parenchymal 3 33 % abnormalities The first group comprised patients with cerebral lacunar infarctions or hypertensive putameno-capsular haemorrhage (33%, See table 1,2). Although these cerebral parenchymal pathologies are not causally related to the existing fusiform aneurysms, however both apparently share common aetiology (hypertensions) and subsequently are occasionally concomitantly present, clinically, in some patients suffering from longstanding essential hypertension. The association between fusiform aneurysms and cerebral lacunar infarctions or hypertensive cerebral haemorrhage is simply a reflection of an association between fusiform aneurysms, as a hypertensive large vessel disease of the intracranial extracerebral arteries, and the hypertensive microvascular (small vessel) brain disease. Metwally, 2001,2008 In microvascular brain disease, the small penetrating arterioles of the subependymal and the pial microvascular systems tend to become stenosed and undergo lipohyalinosis or they may dilate to form microaneurysms (these microaneurysms could be of the berry or the fusiform type), Fisher, 1969, 1972, Hachinski et al, 1987, Tuszynski et al, 1989. From the pathological point of view both Lipohyalinosis and microaneurysms, almost invariably, coexist in
- 5. the same individual, thus making the patient liable to develop either the ischaemic microvascular brain disease (such as lacunar infarctions, leukoaraiosis etc.) or the haemorrhagic microvascular brain disease (such as hypertensive cerebral haemorrhages), Fisher, 1969, 1972, Hachinski et al, 1987. Lacunar infarctions and hypertensive cerebral haemorrhages are two facets of one and the same bad coin (the microvascular brain disease), Hachinski et al, 1987, Tuszynski et al, 1989. It looks like that, in some hypertensive patients, the cerebral small vessel disease is occasionally associated with large vessel disease of the extracerebral intracranial large arteries in the form of quot; fusiform aneurysmsquot;. Intracranial fusiform aneurysms (arterial ectasia) can be regarded as an independent risk factor for microvascular brain disease. However we can not negate the possibility that, at least in some patients, the associated cerebral lacunar infarctions could be the result of microemboli detached from the intraluminal thrombosis that is frequently present in fusiform aneurysms. Schnee and Flamm, 1997, Metwally, 2001,2008 The second group, in the sudy of Metwally 2001 (33%, See table 1,2), comprised patients with brain stem infarctions. Circumferential intraluminal laminated thrombosis is common in fusiform aneurysms and can cause ischemia by directly impairing blood flow or by obscuring the origin of the perforating vessels that supply the brain stem, Schnee and Flamm, 1997. Occlusion of the orifices of branch vessels by thrombosis might be responsible for the brain stem infarctions observed in those patients. Metwally, 2001,2008 Figure 5. Occlusion of the orifices of branch vessels by mural thrombosis might be responsible for the brain stem infarctions observed in patients with fusiform aneurysm. The mass effect of large fusiform aneurysms is probably responsible for the clinical symptomatology observed in 2 patients in the study of Metwally, 2001 (See table 1,2). The clinical picture of those patients actually simulated brain tumours. It is well known that huge fusiform aneurysms can simulate brain tumours both clinically and even on MRI or CT scan, Schnee and Flamm, 1997. In the currently reported case, the fusiform aneurysm grossly indent the brain stem and was actually seen embedding itself deeply into the anterolateral aspect of the brain stem. Metwally, 2001, 2008 A huge ectatic basilar artery may even produce indentation of the floor of the third ventricle, obstruct the foramen of monro, and interference with the circulation of cerebrospinal fluid enough to produce hydrocephalus, Schnee and Flamm, 1997. A greatly elongated and ectatic vertebral artery may press upon cranial nerves and even simulate a cerebellopontine angle tumor clinically and on CT scan and MRI, Gobin et al, 1996, Schnee and Flamm, 1997, Metwally, 2001. Basilar artery aneurysms often imbed themselves deeply in the anterior or anterolateral aspect of the brainstem. Long tract signs are frequently produced, Schnee and Flamm, 1997, Metwally, 2001. The aqueduct of Sylvius may be displaced far backward and narrowed, and the floor of the posterior part of the third ventricle may be invaginated, Schnee and Flamm, 1997. Narrowing of the aqueduct frequently produces hydrocephalus involving the lateral and third ventricles. Gobin et al, 1996, Schnee and Flamm, 1997, Metwally, 2001,2008 In this way arterial ectasia can be regarded as being directly implicated, aetiologically, in clinical symptoms formations either by inducing compression of the nearby neural structures when it is huge enough or by the circumferential intraluminal laminated thrombosis that induces ischemia by directly impairing blood flow or by obscuring the origin of the perforating vessels that supply the brain stem.
- 6. Table 3. In the study of Metwally, 2000, patients with parenchymal involvement were divided into three groups. Group Comment Group I The first group comprised patients with cerebral lacunar infarctions or hypertensive putameno- capsular haemorrhage (33%, See table 1,2). Although these cerebral parenchymal pathologies are Cerebral not causally related to the existing fusiform aneurysms, however both apparently share common lacunar aetiology (hypertensions) and subsequently are occasionally concomitantly present, clinically, in infarctions some patients suffering from longstanding essential hypertension. The association between fusiform or aneurysms and cerebral lacunar infarctions or hypertensive cerebral haemorrhage is simply a hypertensive reflection of an association between fusiform aneurysms, as a hypertensive large vessel disease of putameno- the intracranial extracerebral arteries, and the hypertensive microvascular (small vessel) brain capsular disease. Metwally, 2001,2008 haemorrhage Group II The second group, in the sudy of Metwally 2001 (33%, See table 1,2), comprised patients with brain stem infarctions. Circumferential intraluminal laminated thrombosis is common in fusiform Brain stem aneurysms and can cause ischemia by directly impairing blood flow or by obscuring the origin of infarctions the perforating vessels that supply the brain stem, Schnee and Flamm, 1997. Occlusion of the orifices of branch vessels by thrombosis might be responsible for the brain stem infarctions observed in those patients. Metwally, 2001,2008 Group III A huge ectatic basilar artery may even produce indentation of the floor of the third ventricle, obstruct the foramen of monro, and interference with the circulation of cerebrospinal fluid enough Mass effect to produce hydrocephalus, Schnee and Flamm, 1997. A greatly elongated and ectatic vertebral artery may press upon cranial nerves and even simulate a cerebellopontine angle tumor clinically and on CT scan and MRI, Gobin et al, 1996, Schnee and Flamm, 1997, Metwally, 2001. Basilar artery aneurysms often imbed themselves deeply in the anterior or anterolateral aspect of the brainstem. Long tract signs are frequently produced, Schnee and Flamm, 1997, Metwally, 2001. The aqueduct of Sylvius may be displaced far backward and narrowed, and the floor of the posterior part of the third ventricle may be invaginated, Schnee and Flamm, 1997. Narrowing of the aqueduct frequently produces hydrocephalus involving the lateral and third ventricles. Gobin et al, 1996, Schnee and Flamm, 1997, Metwally, 2001,2008 In a single patient, in the study of metwally 2001, the clinical presentation was in the form of vascular headache indistinguishable from common migraine, in this particular case the fusiform aneurysm was associated with saccular (berry) aneurysm at the tip of the basilar artery. Because vascular headache was not recorded in other patients included in this study (and in fact was not mentioned in any of the literature reviewed as a clinical symptom of fusiform aneurysm) we can say that the vascular headache is caused by the berry aneurysm and not by the associated fusiform aneurysm which could be asymptomatic in this case. Vascular headache is a common symptom in berry aneurysms. The association between berry aneurysms and fusiform aneurysms was mentioned before, william, 1992. This association is, however, extremely uncommon. Schnee and Flamm, 1997 In intracranial arterial ectasia, the basilar artery is the most frequently involved artery and the vertebral arteries are involved next in frequency. Extension of ectasia to other large arteries (such as the carotid arteries, the middle or anterior cerebral arteries) is extremely uncommon. William, 1992. Weir, 1987, Mizutani and Aruga, 1992, Gobin et al, 1996, Schnee and Flamm, 1997, Metwally, 2001,2008 Pathologically mural thrombosis is almost invariably present in fusiform aneurysms, Schnee and Flamm, 1997, thrombosis, however, might not be quite evident on CT scan, MRI or angiography, Setton et al, 1996, Schnee and Flamm, 1997. Thrombosis is probably caused by the rough surface of the aneurysms, Schnee and Flamm, 1997, and by the haemorheological abnormalities ( increased blood viscosity) and the increased thrombotic tendency of the blood (increased fibrinogen level, increased platelet aggregation, increased RBCs aggregation, etc.) that are frequently associated with essential hypertension. Pearson et al, 1981, Schneider et al, 1987, Tuszynski et al, 1989. Repetitive episodes of minute haemorrhages within the wall of these aneurysms were suggested by some authors to be the cause of the laminated mural thrombosis observed inside these aneurysms, Mawad and Klucznik, 1995. Grossly thrombosed aneurysms appear of mixed density on precontrast CT scan with a hypodense lumen that enhances. MRI is superior to CT scan in demonstrating the true size of the aneurysm and in the demonstration of
- 7. mural thrombosis. Atlas, 1997, Schnee and Flamm, 1997, Metwally, 2001 Mural thrombosis might compromise the true size of these aneurysms on angiography, Setton et al, 1996, Bagley and Hurst, 1997, however an estimation of the true size of the aneurysm may be gained from the displacements of adjacent vessels and the circumferential course of the basilar arterial branches around the lesion and the displaced and deformed brainstem, Setton et al, 1996. The double lumen observed by CT scan in one patient, in the sudy of Metwally, 2001, was described before on CT scan, Schnee and Flamm, 1997, and on angiography, Setton et al, 1996, Bagley and Hurst, 1997, it was regarded as due to intraluminal thrombosis. Schnee and Flamm, 1997. Although the double lumen appearance was demonstrated in only one patient, in the sudy of Metwally 2001, however all aneurysms appeared slightly hyperdense on precontrast CT scan in that study and this could be due to the existence of mural thrombosis because when a thrombus or embolus occurs, serum is extruded from the clot producing an increase in the hemoglobin concentration and a subsequent increase in density on precontrast CT scans. Bell, et al, 1985, Bozzao, et al, 1989, Bastianello, et al, 1991, Weller, 1992, Metwally, 2001 Figure 6. Postcontrast CT scan showing basilar artery fusiform aneurysm with the characteristic double lumen. The aneurysm is embedding itself in the brain stem. Figure 7. Precontrast CT scans showing basilar artery fusiform aneurysm, notice the rounded configuration, the midline location in the prepontine cistern, and the precontrast hyperdensity that could be due to thrombosis ( density below that of calcification). This patient was presented with massive pontine-midbrain infarction with the locked in syndrome. Fusiform aneurysms are usually not amenable to endovascular obliteration because they have no neck. Additional endovascular risks include coil compaction with aneurysm recanalization, coil displacement, and delayed, uncontrolled thrombosis progression. Balloons, if used, must be inflated in the proximal arterial segment because of the risk of migration, embolization, or rupture. At present, endovascular coil bracing of fusiform aneurysms should be limited to eccentric pouches when parent artery occlusion is not possible. Operation may be warranted if symptoms progress despite antiplatelet or anticoagulant therapy but carries substantial risk and is technically demanding. Surgical options include proximal ligation, decompressive thrombectomy, resection, and trapping. Vessel reconstruction with a series of clips or vein graft bypass may be indicated, but the loss of small branches along the reconstructed vessel poses a serious risk. Weir, 1987, Mizutani and Aruga, 1992, Gobin et al, 1996, Schnee and Flamm, 1997, Metwally, 2001
- 8. For the management of these patients the following protocol is suggested by us If fusiform aneurysms are accidentally discovered ( for example during radiological examination for other causes) probably nothing should be done to the patient and the patient is better left alone. The role of antiplatelet or anticoagulant therapy to prevent mural thrombosis is yet to be defined. When fusiform aneurysms are associated with ischaemic brain manifestations antiplatelet or anticoagulant should be given in the hope of retarding mural thrombosis which undoubtedly plays a significant role in the pathogenesis of ischemic manifestations. Surgery is probably warranted in case of persistence of ischemic manifestations despite antiplatelet or anticoagulant therapy, however this option must be carried out by surgeons with sufficient experience with this kind of aneurysms. Figure 8. Selective treatment of a fusiform aneurysm of the carotid siphon in a 56-year- old man. (A) Three-dimensional angiography shows the fusiform appearance of the lesion. The aneurysm involves the entire circumference of the vessel, and there is a lateral pouch. (B) Road map image during the treatment performed using remodeling technique for positioning of the coils. (C) Antero–posterior view of the right ICA angiogram shows occlusion of the aneurysm and patent parent artery. Figure 9. Fusiform aneurysm presenting with SAH in a 70-year-old woman with atherosclerotic vascular disease. (A) Angio-CT shows a large aneurysm of the basilar artery associated with calcifications and severe atherosclerotic lesions also on both vertebral arteries. Diffuse atherosclerotic lesions also are observed in other locations, including the right carotid siphon (B), the left carotid bifurcation (C), and the left subclavian artery (D).
- 9. SUMMARY SUMMARY Intracranial fusiform aneurysms Commonly involve the vertebrobasilar system and might extend to involve other arteries around the circle of Willis Involved arteries are diffusely dilated, tortuous, kinked, abnormally prolonged with frequent mural thrombosis and occasional wall calcification. Fusiform aneurysms rarely rupture or produce subarachnoid haemorrhage Fusiform aneurysms are commonly associated with microvascular brain disease The clinical presentation of fusiform aneurysms includes Ischemic manifestations Pressure due to the mass effect of greatly dilated fusiform aneurysms Addendum A new version of this PDF file (with a new case) is uploaded in my web site every week (every Saturday and remains available till Friday.) To download the current version follow the link quot;http://pdf.yassermetwally.com/case.pdfquot;. You can also download the current version from my web site at quot;http://yassermetwally.comquot;. To download the software version of the publication (crow.exe) follow the link: http://neurology.yassermetwally.com/crow.zip The case is also presented as a short case in PDF format, to download the short case follow the link: http://pdf.yassermetwally.com/short.pdf At the end of each year, all the publications are compiled on a single CD-ROM, please contact the author to know more details. Screen resolution is better set at 1024*768 pixel screen area for optimum display REFERENCES References -Anson JA, Lawton MT, Spetzler RF: Characteristics and surgical treatment of dolichoectatic and fusiform aneurysms. J Neurosurg 84:185-193, 1996 -Atlas AW: Magnetic resonance imaging of intracranial aneurysms. Neuroimag Clin North Am 7, 4:803-818, 1997
- 10. -Bagley LJ, Hurst RW: Angiographic evaluation of aneurysms affecting The central nervous system. Neuroimag Clin North Am 7, 4:721-737, 1997 -Bastianello S, Pierallini A, Colonnese C, et al: Hyperdense middle cerebral artery CT sign: Comparison with angiography in the acute phase of ischemic supratentorial infarction. Neuroradiology 33:207-211, 1991 -Bell BA, Symon L, Branston NM: CBF and time thresholds for the formation of ischemic edema, and effect of reperfusion in baboons. J Neurosurg 62:31-41,1985 -Bozzao L, Bastianello S, Fantozzi LM, et al: Correlation of angiographic and sequential CT findings in patients with evolving cerebral infarctions. AJNR Am j Neuroradiol 10:1215-1222,1989 -Fisher CH : The arterial lesions underlying lacunes. Acta neuropathologica (Berlin) 12-1, 1969 -Fisher CH, : Cerebral miliary aneurysms in hypertension. American Journal of pathology 66: 313-319, 1972 -Gobin YP, Vinuela F, Gurian JH, et al: Treatment of large and giant fusiform intracranial aneurysms with Guglielmi detachable coils. f Neurosurg 84:55-62,1996 -Hachinski VC, potter P, Allersk,V H : Leukoaraiosis. Acta neurol. 44: 21-23, 1987 -Mawad ME, Klucznik RP: Giant aneurysms: Radiographic features and endovascular treatment. Am j Neuroradiol 16:1053-1060, 1995 -Metwally MYM, Refaat M: Value of magnetic resonance angiography in cerebrovascular disorders, Ain shams medical journal, Vol 50, Number 1,2,3, pp 505-518, 1999 - Metwally, MYM: Intracranial fusiform aneurysm: Report of 9 case, a clinico-radiological study. Ain Shams medical journal, Vol 52. No 1,2,3. 201-227, 2001 -Metwally, MYM: Textbook of neurimaging, A CD-ROM publication, (Metwally, MYM editor) WEB-CD agency for electronic publishing, version 9.1a January 2008 -Mizutani T, Aruga T: quot;Dolichoectaticquot; intracranial vertebrobasilar dissecting aneurysm. Neurosurgery 31:765- 773, 1992 -Morgagni CB: De sedibus et causis morborum venetiis ex. typog. Remondiniana, book 1, letter 4, case 19, 1769 -Pearson TC, Humphy, PRD, Thomas DJ, : Haematocrit, blood viscosity, cerebral blood flow and vascular occlusion in Low GO, Barbenel JC, Forbes CD (eds). Clinical aspact of blood viscosity and red cell deformability. Springler Verlag - Berlin, Heldolberg, New-York., 1981 -Redekop G, Ferguson G: Intracranial aneurysms. In Carter LP, Spetzler RF, Hamilton MG (eds): Neurovascular Surgery. New York, McGraw-Hill, 1995 -Schnee CL, Flamm ES : Usual aneurysms. Neuroimag Clin North Am 7, 4:803-818, 1997 -Schneider R, Ringelstein EB, Zeumer H, : The role of plasma hyperviscosity in subcortical arteriosclerotic encephalopathy (Binswanger disease) J. neurol 234- 67-73, 1987 -Setton A, Davis Aj, Bose A, et al: Angiography of cerebral aneurysms. Neuroimag Clin North Am 6:705-738, 1996 -Tuszynski ML, Petito C.K, leky DE, : Risk Factors and clinical Findings in pathologically verified Lacunar infarctions. Stroke 20: 990 - 999, 1989 -Weir B: Saccular and non-saccular aneurysms. In Aneurysms Affecting the Nervous System. Baltimore,Williams
- 11. & Wilkins, 1987 -Weller R: Spontaneous intracranial hemorrhage. In Adams J, Duchen L (eds): Greenfield's Neuropathology. New York, Oxford University Press, pp 269-301, 1992 -William AW: Neuroradiology. In Joynt RJ (ed), clinical neurology: J B Lippincott company, Vol I, Chapter 2, pp 1-322, 1992