1. Pharmacology
Autonomic Nervous System: A Pharmacological Perspective
1. What is the difference between afferent and efferent nerve fibres?1
2.How many nerves are involved in a somatic
nerve pathway compared to an autonomic nerve
pathway?2
3.Which part of a sympathetic nerve is myelinated?
3
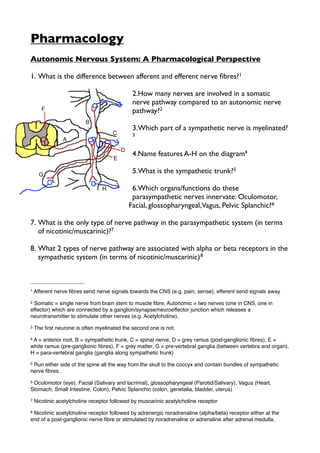
4.Name features A-H on the diagram4
5.What is the sympathetic trunk?5
6.Which organs/functions do these
parasympathetic nerves innervate: Oculomotor,
Facial, glossopharyngeal,Vagus, Pelvic Splanchic?6
7. What is the only type of nerve pathway in the parasympathetic system (in terms
of nicotinic/muscarinic)?7
8. What 2 types of nerve pathway are associated with alpha or beta receptors in the
sympathetic system (in terms of nicotinic/muscarinic) 8
1 Afferent nerve fibres send nerve signals towards the CNS (e.g. pain, sense), efferent send signals away
2Somatic = single nerve from brain stem to muscle fibre, Autonomic = two nerves (one in CNS, one in
effector) which are connected by a ganglion/synapse/neuroeffector junction which releases a
neurotransmitter to stimulate other nerves (e.g. Acetylcholine).
3 The first neurone is often myelinated the second one is not.
4A = anterior root, B = sympathetic trunk, C = spinal nerve, D = grey ramus (post-ganglionic fibres), E =
white ramus (pre-ganglionic fibres), F = grey matter, G = pre-vertebral ganglia (between vertebra and organ),
H = para-vertebral ganglia (ganglia along sympathetic trunk)
5Run either side of the spine all the way from the skull to the coccyx and contain bundles of sympathetic
nerve fibres.
6Oculomotor (eye), Facial (Salivary and lacrimal), glossopharyngeal (Parotid/Salivary), Vagus (Heart,
Stomach, Small Intestine, Colon), Pelvic Splanchic (colon, genetalia, bladder, uterus)
7 Nicotinic acetylcholine receptor followed by muscarinic acetylcholine receptor
8Nicotinic acetylcholine receptor followed by adrenergic noradrenaline (alpha/beta) receptor either at the
end of a post-ganglionic nerve fibre or stimulated by noradrenaline or adrenaline after adrenal medulla.
2. 9. Which sequence occurs in sympathetic nerves other than adrenergic receptors?9
10.By comparison what does a somatic motor neurone look like in terms of
receptors?10
11.Where does the pre-ganglionic cell body tend to be located in the
parasympathetic and sympathetic nerves?11
12.What would an acetylcholine injection do to blood vessels?12
13.What would happen to body functions in the absence of ANS (hexamethonium
man)?13
14.What would happen if you only blocked muscarinic (acetylcholine) receptors?14
15.Which adrenergic receptor affects metabolism?15
16.What are the three main neurotransmitters used in the ‘enteric nervous system’?
16
Receptors: A Pharmacological Perspective
1. What is a receptor and what does it do? 17
9 SNS may be stimulated by nicotinic acetylcholine followed by post-synaptic muscarinic (e.g. sweat)
10A single nerve fibre (no intermediate ganglion) going straight from the CNS to the muscle fibre with a
single nicotinic acetylcholine receptor
11Sympathetic = in thoracic or upper lumbar region (sympathetic trunk), Parasympathetic = brain stem of
sacral (start of Vagus nerve)
12 Would cause vasodilation. Although parasympathetic system does not normally cause vasodilation (except
in the penis) there are vasodilatory acetylcholine receptors in the blood vessels.
13Low blood pressure, vasodilation, reduction of visual accommodation, difficulty in micturation, constipation,
impotence, reduction of various secretions (e.g. sweat)
14All parasympathetic post-ganglionic fibres end in a muscarinic receptor so all parasympathetic function
would be blocked, whereas only sweat glands would be blocked in terms of sympathetic function, since
these are the only muscarinic receptors in the SNS.
15 B2 stimulation leads to release of glucose and fatty acids
16 Acetylcholine, nitric oxide and vasoactive intestinal peptide
17A transmembrane protein (part inside and part outside cell) which serves function of recognition (where a
substance e.g. Ach ʻactivatesʼ the receptor to pass information (transduction) to the cytosol of the cell by
changing shape.
3. 2. What are the shape descriptions of the graph curves showing (i) direct
relationship between drug concentration and number of receptors and (ii) Log of
the drug concentration and number of receptors18
3. What is affinity? 19
4. What is kD? 20
5. What is efficacy?21
6. Why does kD not accurately measure the concentration of drug needed to
trigger a response?22
7. What is the difference between chemical, physiological and pharmacokinetic
antagonism?23
8. What is a non-competitive inhibitor?24
9. What causes a parallel shift to the right in the curve of log concentration against
receptors activated?25
10.What is the dose ratio? 26
11.What is the pA2?27
18 (i) rectangular hyperbolar (ii) sigmoid curve
19 Affinity is how long a reversible drug stays bound to a receptor
20 kD is a measure of a binding substanceʼs affinity. It is the concentration of a drug needed to occupy 50%
of the receptors it occupies at equilibrium. So drugs with a high receptor affinity have a lower kD.
21 The capacity of a drug molecule to induce a response on interaction with a receptor
22kD measures the number of receptors stimulated, it does not account for the efficacy of those receptors so
cannot accurately measure response.
23Chemical is where something direct inactivated another drug, Physiological is where 2 drugs act but each
produce opposing effects and Pharmacokinetic where one alters the way the body handles/metabolises
another
24 Something which inhibits a response by binding to a different binding site (i.e. inhibits without competing
for same binding site as the drug you are trying to inhibit)
25 The presence of a reversible competitive antagonist, since you need a higher dose of the drug to reverse
its effects and maintain a response
26The number of times you need to increase the concentration of agonist to maintain the same response in
the presence of a fixed amount of antagonist.
27(The negative logarithm of the molar concentration of the agonist) which forces you to double to
concentration of agonist to produce same response (e.g. pa2 for propanolol = 8.2). The higher the pa2 the
greater the affinity of the antagonist.
4. 12.What is EC50?28
Intracellular Signaling 1
1.What is a protein kinase?29
2.What is type II diabetes a failure of? 30
3.What is a cell surface ligand interaction?31
4.Label the features A-F on the diagram32
5.Which component of (4) do adenylate cyclase and
phospholipase C activate?33
6.Describe the stages of a signaling pathway using
cyclic AMP34
7.What does phospholipase C initially act on?35
8. What two molecules are released when phospholipase C acts on (7)?36
9. What is released by the 3-phosphate molecule release by phospholipase C? 37
10.What steps might be involved in Ca2+ as a 2nd messenger?38
28 EC50 is a measure of potency of a drug, it is the concentration required for 50% of the max response.
29 An enzyme which is used to transfer phosphate molecules from ATP to a protein molecule
30 Insulin signaling pathway
31 A signaling process which requires both cells to be in direct contact (e.g. T cells receptors). So no need for
ligand to be transported to target cell surface.
32A = ligand, B = receptor, C = adaptor protein, D = 2nd messenger, E = 2nd messenger activates protein
kinase, F = protein kinase and ATP add phosphate to target molecule
33Both activate second messengers (cAMP in the case of adenylate cyclase and DAG in the case of
phospholipase C)
34Receptor --> Adaptor Protein --> Adenylate cyclase and ATP --> Cyclic AMP --> activates Cyclic AMP
dependent protein kinase/protein kinase A --> dissociation of protein kinase --> adds P to target protein
35 Phospholipids within the plasma membrane
36 Phospholipase C acts on plasma phospholipids to release DAG and IP3
37The 3 phosphate molecule is IP3, which binds to IP3 receptors on the ER to release stored calcium. This
could ultimately lead to contraction of the cell.
38 Activation of a calcium calmodulin/calcium-dependent protein kinase) which can act on target molecule
5. 11.How is cyclic GMP generated and what can it do?39
12.How is nitric oxide generated in cells and what is its mechanism?40
13.How is a signal terminated? 41
Intracellular Signaling 2
1. What are the three main classes of membrane receptor?42
2. What does a g-protein bind to?43
3. Describe the process of g-protein signalling44
4. What effect do (i) adrenaline and (ii) CB1 cannabinoid have on levels of cyclic
AMP?45
5. What is the pathway involving cyclic AMP following stimulation of an adrenergic
receptor? 46
6. Describe the process involving adrenaline and/or glucagon which leads to turning
off glycogen synthesis and initiates glycogen breakdown47
39GTP synthesis into cyclic GMP in the presence of guanylate cyclase. It may either control ion channels or
activate cyclic GMP dependent protein kinase
40 Produced from arginine in presence of nitric oxide synthase. Works with guanylate cyclase enzyme and
into cyclic GMP pathway (above).
41 Removal of the initial signal, degradation of the receptor-ligand complex, cell becomes ʻtolerantʼ to signal
and less responsive over time, removal of second messengers by another enzyme or calcium taken to
intracellular stores, de-phosphorylation of activated proteins by protein phosphatase enzymes
421/ G-protein coupled receptors (Cyclic AMP, Glucagon, adrenaline), 2/ Catalytic receptors (insulin,
cytokines), 3/ Inotropic/Ligand gated ion channels (Nicotinic Acetylcholine receptor)
43 either GTP (signal active when bound) or GDP (signal inactive when bound)
44Hormone binds receptor, G-protein associates with receptor, GTP/GDP exchange on G-protein (either
activated or deactivated), G-protein dissociates into alpha and beta subunits, alpha activates effector
enzyme which regulates 2nd messenger production, GTP hydrolysed to GDP and G-protein re-associates.
45Adrenaline increases cyclic AMP and CB1 decreases cyclic AMP because they are linked to different G
proteins which act in different ways.
46GTP binds to alpha subunit, taking over from GDP, alpha subunit breaks off and binds to adenylate
cyclase, activating it. Adenylate cyclase is then able to convert ATP into cyclic AMP.
47cAMP released from b-adrenergic receptor or glucagon receptor, subunit of protein kinase A stimulates
glycogen phosphorylase and blocks glycogen synthase. Similar route for breakdown of triglycerides.
6. 7.What are CB1 receptors? 48
8.The diagram shows the structure of an insulin receptor,
what are the subunits marked A and B? Also, what happens
when the bottom two subunits have a phosphate attached?49
9.What causes autophosphorylation of the tyrosine kinase
domain of an insulin receptor? 50
10.The insulin pathway results in activation of Akt protein
kinase, what does this cause?51
11.A ligand gated ion channel is made up of alpha, beta, gamma and delta sub-units,
which ones does the ligand bind to and what makes the channel ligand gated? 52
12.What substance is released from the nerve terminal in the case of an
acetylcholine receptor to open ligand gated ion channels and what substance
flows through the ligand gated channels?53
Adrenergic Neurotransmission
1. What is a varicosity?54
2. What defines something with an ‘inotropic effect’?55
48 Stands for cannabainoid receptor. It exchanges GDP for GTP on its alpha subunit (same as before) BUT
binds to adenylate cyclase and DEACTIVATES it as opposed to activating it, purely because the GTP binds
to a different area of the alpha subunit.
49A = 4x alpha subunits, where insulin binds, B = 2x beta subunits, where tyrosine kinase can add a
phosphate to increase kinase activity towards substrates.
50 Binding of insulin to insulin binding domain
51 Akt protein kinase causes Glut4 vesicles to translocate to the cell membrane, these allow glucose to pass
through the membrane in the form of glucose-6-phosphate. Also causes glycogen synthase to be released
from inhibition by glycogen synthase kinase allowing it to convert glucose-6-phosphate into glycogen.
52 Ligand binds to the alpha sub-units causing them to change alignment in relation to other polar molecules
lining the central pore, increasing the size of the gap between them and opening the channel.
53
Acetylcholine released from nerve terminals, binding and causing ligand gated channels to open, allowing
Na+ ions to diffuse into the cell and start membrane depolarisation and action potential.
54 A swelling or raised area in the sympathetic nerve from which noradrenaline is released as a transmitter
55 It has an effect on the cardiovascular system to increase force, stroke volume, heart rate and contractility
7. 3. What primary effect does sympathetic stimulation (adrenaline and noradrenaline)
have on: the gut, bladder, sexual function, salivary glands, eye, respiratory system,
skin and metabolism?56
4. What is the difference between a-adrenergic receptors and b-adrenergic
receptors?57
5. What do each of a1, a2, b1 and b2 receptors do when stimulated, are they
presynaptic or post-synaptic? 58
6. Describe the cycle/route of noradrenaline as a transmitter from the sympathetic
varicosities.59
7. What are ‘indirect sympathomimetics’? 60
8. What are ‘direct sympathomimetics’? 61
9. Which beta receptors respond to the b-selective drugs (i) Isoprenaline (ii)
Salbutamol (iii) Dobutamine62
10.What might a selective a1 blocker be used for?63
Lung Mechanics 1 - Compliance and Surfactant
56the gut (decreased blood supply), bladder (inhibition of urination), sexual function (ejaculation,
detumescence (‘party over’)), salivary glands (saliva thickens), eye (pupil dilation), respiratory system
(bronchodilation), skin (decreased blood flow, sweating) and metabolism (release of glycogen, fatty acid
metabolism, increased blood glucose)
57 A = mainly stimulated by noradrenaline, B = mainly stimulated by adrenaline
58A1 (post-synaptic) = vasoconstriction of coronary arteries and veins, decreased motility in GI tract, A2 (pre-
synaptic) = inhibit noradrenaline release, some vasoconstriction, B1 (post-synaptic) = Increased HR and
contractiliy, B2 (non-synaptic) = bronchodilation, vasodilation, glycogen mobilisation
59 Once noradrenaline has been released and has acted, about 80% of it is reabsorbed into the varicosity by
a process called uptake 1, many drugs including cocaine and antidepressants inhibit this mechanism, so
noradrenaline is longer-acting. The 20% that does not get reclaimed by uptake 1/neuronal uptake is
metabolized in the tissue by COMT and further metabolized in the liver and gut to VMA which is excreted,
this can be measured in the urine as a test of sympathetic nervous activity.
60Drugs which cause competitive inhibition of uptake 1 by ʻhikackingʼ the uptake. This process also causes
noradrenaline to be displaced from its storage cells, forcing it out of the sympathetic nerve and activating it.
Examples include tyramine (found in blue cheese, red wine and and anything with yeast).
61The actual transmitters themselves when they are used as a drug. Noradrenaline and adrenaline are
widely used in emergency cardiac treatment.
62(i) Isoprenaline - B1 and B2, used as treatment for heart block (ii) Salbutamol - B2 only, used to treat
bronchoconstriction in asthma (iii) Dobutamine - B1 only, used to increase CO in cardiogenic shock
63A1 blockers are occasionally used as antihypertensives, a1 selective blockers such as prazosin do not
cause tachycardia like non-selective alpha blockers (as a2 inhibited noradrenaline builds up).
8. 1. What is the purpose of surfactant?64
2. What type of cells produce surfactant?65
3. What is elastic resistance? 66
4. What is airway resistance? 67
5. What is transudation? 68
6. What is alveolar interdependency? 69
7. In an alveolus with a fixed number of surfactant molecules, what will happen to
surface tension as expiration forces the alveolus to shrink? 70
8. What is neonatal respiratory distress syndrome? 71
9. What are the effects of chronic bronchitis on the airways and alveoli? 72
10.What are the effects of reversible asthma on the airways and alveoli?73
11.What are the effects of emphysema on the airways and alveoli?74
12.Clinically, how can intrapleural pressure be measured? 75
64Surfactant opposes the tendency for alveoli (spherical structures) to collapse, they also reduce the
pressure by doing this which also reduces the tendency to suck fluid into the alveoli (transduction)
65 Type II pneumocytes
66 Resistance to stretch of the lung tissues and air-liquid interface lining the alveoli
67 Resistance due to friction between layers of flowing air and between the air and the airways
68 The tendency to suck fluid into alveoli during exhalation, surfactant prevents this from happening
69 Joining of alveoli to each other as you breath out, holding them together helps alveoli resist collapse
70 As alveolus shrinks the surface concentration per unit of area of surfactant rises, so surface tension drops
71 Neonatal Respiratory Distress Syndrome (absence of surfactant in lungs), if baby is premature it is quite
likely to lack the ability to produce surfactant. Increased work of breathing, areas of lung collapse, overall
reduction in compliance.
72 Chronic bronchitis = hypertrophied glands and mucus but normal alveoli
73 Asthma = mucosal edema and bronchoconstriction but normal alveoli, does not usually affect compliance
74 Emphysema = high lung compliance so airways become poorly supported and alveoli are destroyed
75Oesophageal balloon, spirometer (lung volume). Intrapleural pressure is negative when no air is flowing,
so effort is involved in pushing air out of the lungs.
9. 13.Give an example of a disease that causes low compliance/stiff lungs and one that
causes high compliance/floppy lungs76
14.In someone with stiff lungs, what would happen to FEV177?
15.What happens to FRC in lungs with (i) high compliance, (ii) low compliance78
Lung Mechanics 2 - Airway Resistance
1.What factors affect airway resistance? 79
2.Anatomically, what are the main sites of airway resistance?80
3. What factors affect bronchial smooth muscle tone?81
4. Which parts of the airway does COPD damage?
5. What is ‘dynamic compression’ of airways?82
6. What generates wheezes in disease or exercise?
7. Explain the phenomenon of ‘air trapping’83
76Low compliance (lack of surfactant?) = Neonatal Respiratory Distress Syndrome or COPD, High
compliance = emphysema
77FEV1 = Forced expiratory volume in 1 second, stiff lungs would have a high elastic recoil so in theory this
should be higher than normal, but stiff lungs also means lungs are smaller as they are sucked in on
themselves so the overall size of the lungs is less, meaning FEV1 is lower than normal.
78Functional residual capacity is the volume left in the lungs after a full forced breath out. High compliance =
increased FRC because of the ʻbarrel chestʼ effect, patients with this condition are breathing at overall larger
lung volumes. In low compliance, the FRC is smaller because the overall size of the lungs is smaller.
79Main factor in the clinical setting is airway radius (halving airway radius gives 16x increase in resistance).
The main things which change radius are mucus, muscle tone, inflammation, hypertrophy of glands.
80nose, pharynx, larynx and medium sized bronchi. Generation 3 bronchi are the greatest, further down
there is a lower radius per bronchiole but more in parallel
81 Main factors affecting bronchial SM tone are: sympathetic nervous system (adrenaline stimulates B2
receptors to relax tone), vagal stimulation (relax or constrict), inflammatory reactions (prostaglandins (can
dilate or constrict, constrict in this case), leukotrienes, histamine),
82 Dynamic compression is where we raise intra-pleural and therefore alveolar pressure due to abdominal
muscle constriction (breathing out). The airways are most likely to collapse are bronchi generation 3 or 4
(site of highest resistance). Fast breathing out at low lung volume however is effort independent.
83In COPD, airways are collapsible so forced expiration is effort independent at higher lung volumes as well
as lower ones. Air trapping as middle airways collapse, breath out cannot be completed, lungs gradually
expand (chest expands during bad asthma attack).
10. 8. What is a normal relationship between FEV and FEV1? 84
9. What happens to FEV1, FVC and FEV1:FVC ratio in restrictive lung disease? 85
10. What happens to FEV1, FVC and FEV1:FVC ratio in obstructive lung disease?86
84 Normally FEV1 is 75% of FVC normal FVC can be 4-6L
85Restrictive lung disease = FEV1 greatly decreased, FVC decreased and FEV1/FVC normal (i.e. FEV1
75% FVC), because lungs are smaller.
86Obstructive airway disease = FEV1 greatly reduced, FVC decreased and FEV1/FVC decreased because it
takes longer to get your vital capacity out.