3. Why 5 cm above LES?
• Has been standard for many years
• Chosen to avoid catheter migration into stomach
• Moving by a 1 cm or two would not change results
• Moving it 10 cm above LES miss a number of patients
who are identified by the more distal location
4. Location of LES
• Manometric localization Reference method
• pH step-up method Sudden rise to pH > 4
• LES locator Prior to pH
• Fluoroscopic techniques Not accurate
• Endoscoic technique Not accurate
5. Why pH < 4?
• Defined early in development of the technology
• Its choice was based on:
- Marked difference from normal esophageal pH of 7
- Pepsinogen converted to pepsin at pH 4
- pH < 4 was one that tends to produce symptoms
• Some believe that drops in pH that do not reach level
of 4.0 still may represent reflux that these events
should also be used in calculations of indices
6. Composite scoring systems
Johnson & DeMeester is the most commonly used
Percentage of total time pH < 4
Percentage of upright time pH < 4
Percentage of supine time pH < 4
Number of reflux episodes
Number of reflux episodes >5 min
Longest reflux episode
DeMeester score
Normal < 14,72
7. Normal values of DeMeester’s score
50 healthy volunteers
DeMeester TR et al. Ann Surg 1976 ; 184 :459 – 470.
8. Normal 24 hours esophageal pH monitoring
Composite DeMeester score: 8.4
DeMeester normal < 14.72 (95th percentile)
Bremner CG et al. Esophageal disease & testing. Taylor & Francis Group, 2005.
9. Qualitative analysis
Symptom–reflux correlation
• Symptom index: Positive if ≥ 50%
• Symptom sensitivity index: Positive if > 10 %
• Symptom association probability Positive if > 95%
Determine relationship between heartburn episodes & acid
reflux events, regardless if pH test is normal or abnormal
12. Symptom Association Probability Calculation
Positive if 95%
• Divides tracing into 2-min segments & looks at
whether a symptom & acid are present during each 2
minute segment
• The analysis uses contingency table analysis of 4
possible outcomes for each segment:
acid + symptom +
acid + symptom –
acid – symptom +
acid – symptom –
13. Overall amount of acid exposure & number of
reflux episodes are the focus of many studies
using ambulatory pH testing
Relationship between symptoms & esophageal
acid is equally (or perhaps more) important
14. 24 hours pH monitoring & medications
• PPI should be stopped for 5 – 7 days
• Other medications should be stopped for 1 – 3 days
• Patient must not use antacids or other OTC
medications for duration of the study
15. 24 hour pH esophageal monitoring
On & off therapy
• Off therapy
Uncertainty about diagnosis of reflux
Mildest grades of esophagitis: redness - friability
Very short segments of BE
• On therapy
Patient who has failed a therapeutic trial
Patient has known reflux or highly likely to have reflux
pH probe in esophagus & another in stomach (NAB)
16. Percentage of total time pH < 4
Normal values
• Off therapy
5 cm above LES
20 cm above LES 1 %
Periods of meals or acidic beverages excluded
• On therapy
5 cm above LES
20 cm above LES ?
* Based on 95% CI obtained in healthy subjects treated with omeprazole 40 mg qd
Kuo B et al. Am J Gastroenterol 1996 ; 91 : 1532 – 8.
4 – 5.5 %
1.6 – 4 %*
18. Principle of “MII”
• 2 steel rings separated by isolator
• Alternating-current generator to apply electrical PD
• Circuit closed through electrical charges (ions)
contained in structures surrounding the catheter
Gastrointest Endoscopy Clin N Am 2005 ; 15 : 257 – 264.
19. Impedance scale
Refluxate: High conductivity & low impedance
Air: Low conductivity & high impedance
Bremner CG et al. Esophageal disease & testing.
Taylor & Francis Group, New York, 1st edition, 2005.
20. Advantages of MII
• Content of refluxate Liquid – Gas – Mixed
• Direction of bolus Anterograde – retrograde
• Height of refluxate
• pH characteristics Acid
(combined MII-pH) Weekly acid
Weekly alkaline
Acid re-reflux
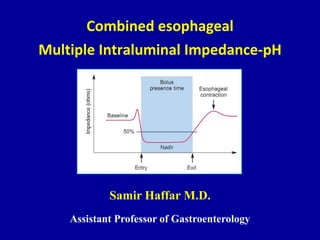
21. Liquid bolus
Gastrointest Endoscopy Clin N Am 2005 ; 15 : 257 – 264.
1) Initial drop Liquid enters impedance-measuring segment
2) Rise Bolus cleared from this segment
3) Overshoot Decreased luminal cross-section during contraction
4) Return to baseline
22. Air bolus
(Belch, Air swallow)
1) Rapid rise Presence of air bolus inside esophagus
2) Rapid decrease Air bolus clears from this segment
Gastrointest Endoscopy Clin N Am 2005 ; 15 : 257 - 264.
23. Mixed air – liquid Bolus
1) Rapid Rise Air in front of the bolus
2) Rapid drop Liquid component of mixed bolus
3) Rise Liquid being cleared from this segment
4) Return to baseline
Gastrointest Endoscopy Clin N Am 2005 ; 15 : 257 – 264.
24. Antegrade bolus movement (MII)
Observed during swallowing
Progression of impedance from proximal to distal
Gastrointest Endoscopy Clin N Am 2005 ; 15 : 257 – 264.
25. Retrograde bolus movement (MII)
Observed in reflux
Progression of impedance from distal to proximal
Gastrointest Endoscopy Clin N Am 2005 ; 15 : 257 – 264.
26. Combined MII
• MII used clinically only in combination
– With esophageal manometry (MII-EM)
– With pH (MII-pH)
• MII not considered as replacement for manometry &
pH techniques but as complementary procedure that
expands diagnostic potential of esophageal function
testing & reflux monitoring
27. Combined MII-pH probe
• Impedance orifices
3, 5, 7, 9, 15, & 17 cm from the tip
• pH orifice
5 cm from the tip
• MII-pH probe = pH probe
Do not change patient comfort
Bremner CG et al. Esophageal disease & testing.
Taylor & Francis Group, NY, 1st edition, 2005.
28. “Sleuth” monitor – Sandhill
“Sleuth” monitor attached to the catheter
& worn around a belt during the recording period
29. GERD classification by combined MII-pH
Acid reflux
Reflux with drop of pH from above 4.0 to below 4.0
Superimposed acid reflux (Acid re-reflux)
Acid reflux occurs while pH < 4.0
Weakly acidic reflux
Reflux results in esophageal pH between 4.0 & 7.0
Weakly alkaline reflux
Reflux with nadir esophageal pH does not drop < 7.0
Sifrim D et al. Gut 2004 ; 53 ; 1024 – 1031.
31. GERD classification by combined MII-pH
Acid reflux
Reflux with drop of pH from above 4.0 to below 4.0
Superimposed acid reflux (Acid re-reflux)
Acid reflux occurs while pH < 4.0
Weakly acidic reflux
Reflux results in esophageal pH between 4.0 & 7.0
Weakly alkaline reflux
Reflux with nadir esophageal pH does not drop < 7.0
Sifrim D et al. Gut 2004 ; 53 ; 1024 – 1031.
33. GERD classification by combined MII-pH
Acid reflux
Reflux with drop of pH from above 4.0 to below 4.0
Superimposed acid reflux (Acid re-reflux)
Acid reflux occurs while pH < 4.0
Weakly acidic reflux
Reflux results in esophageal pH between 4.0 & 7.0
Weakly alkaline reflux
Reflux with nadir esophageal pH does not drop < 7.0
Sifrim D et al. Gut 2004 ; 53 ; 1024 – 1031.
34. Weakly acidic reflux (MII-pH)
Gastrointest Endoscopy Clin N Am 2005 ; 15 : 361 – 371.
35. GERD classification by combined MII-pH
Acid reflux
Reflux with drop of pH from above 4.0 to below 4.0
Superimposed acid reflux (Acid re-reflux)
Acid reflux occurs while pH < 4.0
Weakly acidic reflux
Reflux results in esophageal pH between 4.0 & 7.0
Weakly alkaline reflux
Reflux with nadir esophageal pH does not drop < 7.0
Sifrim D et al. Gut 2004 ; 53 ; 1024 – 1031.
37. Recommendations for MII-pH monitoring
• Endoscopy-negative patients with heartburn or
regurgitation despite PPI & performed on PPI therapy
• Utility of impedance in refractory reflux patients with
chest pain or extraesophageal symptoms unproven
• Current interpretation relies on SI, SSI or SAP
• Therapeutic implications of abnormal test unproven
ACG Practice Guidelines: Esophageal reflux testing.
Am J Gastroenterol 2007 ; 102 : 668 – 685.
38. Advantages of 3 major types of pH testing
pH Tubeless Combined
MII-pH
Comfort _ + _
Monitoring > 24 h _ + _
Nonacid reflux _ _ +
Normal values + _ _
Proximal reflux + ? +
Gastric monitoring + ? +
Intragastric pH Monitoring:The evidence supporting the clinical significance and applicability of gastric pH monitoring is insufficient to recommend its routine use inclinical practice.Proximal pH Recording:available evidence does not support the routine use of proximal pH monitoring in clinical practice.
Relatively new technique developed in early 1990s at Helmholtz Institute in Aachen (Germany)Silny* provided first description of this technique that assesses intraluminal bolus movement by measuring changes in conductivity of intraluminal content
A recent, multicenter study examined the impedance characteristics of 60 healthy subjects during 24-h ambulatory monitoring. Based on impedance values 5 cm above the LES, the median number of total reflux episodes per 24 h was 30, the majority of which occurred in the upright position.Approximately two-thirds of the episodes were acid and another third weakly acidic reflux. Weakly alkaline reflux was distinctly uncommon in this healthy cohort. Similar frequencies were recently reported from a multicenter European study. References:Shay S, Tutuian R, Sifrim D, et al. Twenty-four hour ambulatory simultaneous impedance and pH monitoring: A multicenter report of normal values from 60 healthy volunteers. Am J Gastroenterol 2004;99:1037–43.Zerbib F, Bruley des Barannes S, Roman S, et al. 24 hour ambulatory esophageal multichannel intraluminal impedance-pH in healthy European subjects. Gastroenterology 2005;128:A396.