Call Girls Rishikesh Just Call 8250077686 Top Class Call Girl Service Available
Palmer Center for Chiropractic Research-2008
1. Combination of HVLA manipulation, exercise and physical therapy for treatment of Lateral epicondylitis
Mohsen Radpasand, DC, MD
Palmer Center for Chiropractic Research, Davenport, IA, USA
Background
Over View
Lateral epicondylitis, also known as tennis elbow is
defined as pain over the lateral aspect of the elbow
which is aggravated by active wrist extension and
direct palpation over either the lateral epicondyle of
the humerus, the radio-humeral joint space or the
proximal muscle bellies. The incidence and
prevalence is approximately 1%-3%. Women are
more often affected than men, of 9% and 3%
respectively, with a peak prevalence at age 42-44..
At least 40 different treatment modalities aiming to
reduce pain and increase function have been
described, but the optimal treatment remains
undefined.
Supine position, for 10 minutes with the positive
pad was over the lateral epicondyle and the
negative pad was at the base of involved elbow’s
scapula, on the back of the patient. The
stimulations were set to patient’s pain tolerance.
Methods
A systematic 10-week multimodal conservative
management for chronic lateral epicondylitis in a
specific sequence, utilizing quick thrust manipulation,
High-voltage pulse galvanic stimulation (HVPGS),
bracing, ice, exercises, along with restricted usage of
the affected elbow. We used Patient Rated Tennis
Elbow Questionnaire (PRTEQ) as an out come
measure. PRTEQ is a simple reliable, valid, and
sensitive assessment
D) Putty Therapeutic
The arm and forearm should make a 90° angle with
each other, with the wrist extended as far as it can,
while holding the putty. The putty will be pushed
toward the thenar surface of the palm of the hand by
flexing the four digits of 2 to 5 as hard as possible.
Brace
Result
Placed the knob of hard-padded elbow
brace exactly on top of the most painful
area, and wear it between the treatments
ice
Applied over the most painful area
(the lateral epicondyle). The ice size
was small, just to cover the lateral
epicondyle
Introduction
In January of 2007, a 57-year-old female
science teacher reported to our office with chief
complaint of right elbow pain. She complained of
whole arm pain down to the wrist for the past 5
months. She related the pain to her active daily
routines in and around the house, and her daily
exercises. Upon examination her right elbow had
severe palpatory tenderness and pain over region
of the lateral epicondyle. In addition, pain in the
region of the lateral epicondyle during resisted
extension of the middle finger (Maudsley's test)
was present. The ROM and orthopedic tests were
normal. Plain film x-ray was unremarkable.
HVPGS
Exercise
Isometric end point contraction
A) Forearm Extensor
Muscle
The HVLA manipulation
Delivered as a quick thrust using the pad of the thumb in
a posterior to anterior direction over the posterior aspect
of the radial head, approximately on top of the extensor
tendon attachment to the lateral epicondyle. The patient
sat on a chair with the upper body in postural alignment.
The provider’s opposite hand holds the dorsum of the
patient’s wrist. The provider starts with the elbow slightly
flexed, takes it to full extension and applies the thrust at
the end-range while extending the elbow and pronating
the forearm
Has two parts 1) pure extension
at the wrist, 2) radial deviation
and extension
B) Forearm Flexor
Muscle
Has two parts 1) pure flexion
at the wrist, 2) radial
deviation, and flexion
C) Exercise for Supinator and
Pronator Muscle
The participant has the full active
control of the weight. The elbow is
supported at the edge of the table,
while the arm and forearm make a 90°
angle. All of the exercises had duration
per repetition of 10s, with 10
repetitions maximum.
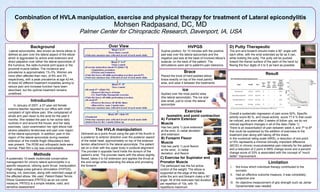
Overall a systematic regression of pain score 52%, Specific
activity score 80 %, and Usual activity score 77.5 % that could
be noticed, and even after 3 weeks of follow ups, we do not
noticed significant changes in all of the data (Table 1).
There is an exacerbation of pain between week 4, and 7th to 8th
that could be explained by the addition of exercises to the
treatment plan along with taking off the brace.
In the numerical rating scale (NRS), a reduction of one point
or15% represents a minimal clinically important difference
(MCID) in chronic musculoskeletal pain intensity for the patient,
and a reduction of 2 point in NRS change score and a percent
change score of 33% is associated with the concept of “much
better” improvement.
Limitation
I.
Not know which individual therapy contributed to the
success
II. Had an effective outcome measure, it was completely
subjective one
III. An objective measurement of grip strength such as Jamar
Dynamometer was needed