Coagulation Monitoring in Critical Care
•Als PPT, PDF herunterladen•
23 gefällt mir•3,851 views

Bench to Bedside

Empfohlen
Empfohlen
Weitere ähnliche Inhalte
Was ist angesagt?
Was ist angesagt? (20)
Andere mochten auch
Andere mochten auch (20)
Ähnlich wie Coagulation Monitoring in Critical Care
Ähnlich wie Coagulation Monitoring in Critical Care (20)
Kürzlich hochgeladen
Kürzlich hochgeladen (20)
Coagulation Monitoring in Critical Care
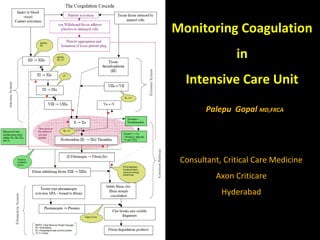
- 1. Monitoring Coagulation in Intensive Care Unit Palepu Gopal MD,FRCA Consultant, Critical Care Medicine Axon Criticare Hyderabad
- 2. Coagulation Monitoring Bleeding Clotting
- 3. Why Monitor Coagulation in ICU Routine ? Coagulopathy Sepsis DIC & Thrombocytopaenia Liver Disease Trauma Post-Surgical CABG On Pro-coagulants Correct Coagulopathy On Anticoagulants and/or Antiplatelets DVT Prophylaxis Anti-thrombotic treatment CAD Thrombolysis Coronary stents Arrhythmias CVA Extracorporeal devices IABP,RRT, MARS, ECMO On Anti-fibrinolytics
- 4. Laboratory Based Coagulation Tests Non-Viscoelastic Tests Issues: 1. Sampling to Results Delay 2. Plasma Values rather than whole blood 3. No information on Platelet function 4. Performed at standard room temperature
- 5. Techniques & Advantages • Full blood count and Coagulation screen (TT, APTT, PT, and fibrinogen) – Quick, easy, reproducible, understandable • Whole Blood tests No sample preparation – Microaggregation, Thrombelastography, & WB analysers – Easy • Purified Platelet tests – Microaggregation Easy – Macroaggregation Precise defect – Platelet function analysers Precise defect • Skin bleeding time – Whole body answer
- 6. Limitations of Techniques • Full blood count – Number not function • Coagulation screen (TT, APTT, PT, and fibrinogen) – 20 to 30 minutes, no fibrinolytic assessment • Whole Blood tests – Microaggregation No commercial kit • Purified Platelet tests • Have to prepare the sample – Microaggregation No commercial kit – Macroaggregation Experienced technician – Platelet function analysers ? • Skin bleeding time – Invasive, not specific
- 7. Tests of Coagulation - Platelets Quantitative Measure Automated cell counters or Mannual Laser technology or Automated flow cytology Platelet Function Tests Static Tests β –hromboglobulin, ADP release, No of surface receptors Dynamic Tests Bleeding Time VEPOC Tests ( TEG / ROTEM / Sonoclot ) Platelet Response to Stimuli Ultegra PLT response to Thrombin Receptor agonist Peptide( TRAP) useful in GPIIb / III a inhibitors Clot Signature analyzer CPB related PLT function Platelet function Analyzer PFA 100 Platelet Works Coulter counter with antagonist Platelet aggregometry Photo-optical instrument Fibrinogen Concentration Clottable Protein method (Clauss method) End-point detection technique Haemochron POC Technique Immunochemical tests Normal 180 -220 mg / dL
- 8. Thrombin Time Time taken for conversion of Fibrinogen to Fibrin Technidyne POC test Normal Whole Blood 39 - 53 secs Citrated Blood 43 -63 secs Specifically measures activity of Thrombin Sensitive to Heparin Excludes Intrinsic & Extrinsic pathway Elevated In Heparin Presence Hypofibrinogenamia Dysfibrinogenaemia Amyloidosis Thrombin Antibodies Appropriate test for Thrombolytics Prolongation by 1.5 – 5 times Effective Therapy Prolongation by > 7 times Risk of bleeding Absence of Prolongation Failed Fibrinolysis
- 9. Activated Partial Thromboplastin Time Tests Intrinsic and Final Coagulation pathway Thromboplastin is Tissue factor + Phospholipids Activated with kaolin (celite-diamataceous-earth) Prolonged with even low dose heparin Prolonged aPTT in Deficiencies of Factors XII,XI,IX,VIII HMW Kininogen Kallikrein Normal Value 28 -32 secs
- 10. Prothrombin Time Tests Extrinsic and common Coagulation pathway PT elevated in Deficiency of Factor VII Deficiency of Vit K Warfarin therapy Monitor heparin / Warfarin crossover Normal PT values 12 – 14 secs International Normalized Ratio (INR) = (PT patient / PT mean normal) ISI ISI = international Sensitivity Index INR target ranges are specified by patient populations DVT, AF INR= 2.0 - 3.0 Mitral mechanical heart valve INR= 2.5 – 3.5 Hypercoagulable disorders INR= 1.5 – 2.5
- 11. Non-Viscoelastic POC Monitors PT & aPTT Coagucheck ( Roche) Hemochron (ITC) Ciba Corning Biotrack 512 Good correlation with Lab values Reiner JS:CCD 1994: 32(1) Been used in Transfusion algorithms Coagucheck Hemochron
- 12. Fibrinolysis Primary & Secondary fibrinolysis Direct Measurement Clot Lysis Time End Product Measurement FDP d - dimers
- 13. Unfractionated Heparin (UFH) • Exerts its anticoagulant effect via antithrombin • Heparin binds to and produces a conformational change in antithrombin. • Anticoagulant effect reversed with protamine.
- 14. UFH - Monitoring • Heparin Concentration – Not standardized • Hepcon POC for WB Heparin concentration • Activated clotting time (ACT) • ACT POC test used for high doses heparin therapy • Lab aPTT stronger correlation to Heparin con. than POC aPTT and ACT Ann Pharmacother 2002;36:7-11 High dose Thrombin Time (HiTT) Hemochron
- 15. LMWH • Binds to antithrombin and inactivates thrombin to a lesser extent than UFH because the smaller molecule fragments cannot bind thrombin and antithrombin simultaneously.
- 16. LMWH – Monitoring Anti-Xa assay is generally used Limitations Not been demonstrated to be good predictor of - Bleeding Risk - Antithrombotic efficacy Relative anti-Xa and anti-IIa activities vary between preparations Antithrombin activity more important in Kinetic studies Comparability of anti-Xa chromogenic assays is poor Assays should be LMWH, method and equipment specific. Thromb Haemost 2002;87:163-164
- 17. Point of Care Coagulation Monitoring (POC) Viscoelastic Point of Care Tests Advantages: 1. Bedside – faster turnaround time 2. Coagulation status of whole blood 3. Clot development in real time 4. Performed at patient’s temperature 5. Therauptic agents added However: In vitro vs in vivo differences Lack of standardization Coagulation under static cuvette conditions (no flow) Non-laboratory personnel
- 18. Viscoelastic POC Devises (VEPOCD) Thromboelastography Rotation TE ROTEM Sonoclot 1.Rotating Cup with Blood 2.Activator/ Inhibitor 3.Pin & Torsion wire 4.Electromech transducer 5.Data Processor 1.Cuvette with Blood 2.Pipette with activator/ Inhibitor 3.Pin & Rotating Axis 4.EM & Light source, Mirror 5.Data Processor 1.Cuvette with Blood 2.Activator/ Inhibitor 3.Disp plastic probe 4.EM Transducer 5.Data Processor
- 19. Sonoclot Tests : Reference Values Entire Haemostasis Sonoclot Assay SonACT kACT gbACT aiACT Activated Clotting Time 85 -1 45 s 94 -178 s 119-195 s 62 -93 s (ACT) Clot Rate (CR) 15 – 45 15 -33 7 -23 22 – 41 U / min U / min U / min U / min Low dose Heparin Overall coag & PLT function PF 0 - 5 Qualitative Graph Qualitative Graph ACT CR PF
- 20. TEG & ROTEM Display TEG ROTEM
- 21. Tests of Viscoelastic POC Devices Assay Activator/ Inhibitor Indication & Assessment TEG Native None Custom Haemostsis test Kaolin Kaolin Overall coagulation & PLT Function Heparinase Kaolin+Heparinase Specific detection of Heparin Platelet Mapping ADP Arachidonic acid PLT Function, Monitoring anti-PLT therapy ROTEM Na-TEM None Custom Haemostsis test ex-TEM Tissue Factor Extrinsic PW, Clot Formation & Fibrinolysis in-TEM Contact activator Intrinsic PW, Clot formation &Fibrin Polymeriz fib-TEM TF+ PLT Antagonist Qualitative assessment of Fibrinogen level ap-TEM TF+Aprotinin Fibrinolytic PW + Fibrinolysis Hep –TEM CA+ Heparinase Detection of Heparin eca-TEM Ecarin Management of Direct Thrombin Inhibitors tif-TEM 1:1000 TF Ex PW:monitoring rF VIIa Sonoclot Native None Custom Haemostsis test gbACT Glass Beads Overall coagulation & PLT function H-gbACT Glass beads + Heparinase + Presence of Heparin microPT 1:1000 TF Ex PW:monitoring rF VIIa SonACT Celite Large dose Heparin without Aprotinin kACT Kaolin Large dose Heparin +/- Aprotinin aiACT Celite+Clay Large dose Heparin with Aprotinin
- 22. Nomenclature & Reference Values of TEG & ROTEM TEG ROTEM Clotting Time R(reaction Time) CT(clotting Time) Period to 2 mm amplitude N(WB) 4 – 8 mins N(Cit,in-TEM) 137-246 secs N(Cit,Kaolin) 3- 8 mins N (Cit, ex-TEM) 42 – 74 secs Clot kinetics K (kinetics) CFT (Clot formation time) Period from 2 to 20 mm N (WB) 1- 4 mins N (Cit,in-TEM) 40 -100 secs N(Cit,Kaolin) 1-3 mins N (Cit, ex-TEM46 -148 secs Clot strengthening α (slope between r & k) α (slope of tangent at 2mm ampli) (Alpha angle) N(WB) 470 to 740 N (Cit,in-TEM) 710 -820 N(Cit,kaolin) 550 780 N (Cit, ex-TEM) 630 -810 Amplitude A A (at set time) MA(maximum amplitude) MCF (maximum clot firmness) N (WB) 55 -73 MM N (Cit,in-TEM) 52 – 72 mm N(Cit,kaolin) 51 -69 mm N (Cit, ex-TEM) 9 -25 mm Lysis (at fixed time) CL30, CL 60 LY30,LY60
- 23. TEG / ROTEM POC Coagulation Monitoring in ICU Post Cardiac Surgery Reduce Transfusion requirement in adults & children Spalding GJ : Cardiothoracic Surg:2007 :31-1052 Heparinase TEG based algorithm – ↓Transfusion Royston D:BJA 2001: 86-575 Novel TEG based ACT Chavez JJ Anesth Analg 2004:99:1290 Hepatology CLD & ALF - Defective synthesis & Hyperfibrinolysis Post OLT – Haemorrhagic, Hypercoagulable & Thrombotic Coakley M,J CT Vasc Anaesth2006:20:548 Hypercoagulability Short R/CT time & Increased MA/MCF Mc Crath DJ: Anaesth Analg 2005;100:1576 Trauma Trauma related coagulopathy Obstetrics PET + HEELP
- 24. TESGt &an RdOaTrEdM T DEiGsp Ilmayages
- 25. Monitoring Anticoagulant Therapy Heparin Therapy VEPOCD ACT VEPOCD with Heparinase LMWH & Heparinoids Danaparoid Corpel JA Haemophelia 2005 Direct Thrombin Inhibitors Hirudin, Bivaluridin, Argobatron, Ximelagatran For ACS, VTE & HITS VEPOCD with Ecarin Clotting Time Caroll RC Anaesth Analg: 2006: 102: 1316
- 26. Monitoring Procoagulant Therapy Specific component Therapy Fibrinogen levels MCF / MA of VEPOCD Antifibrinolytic drugs Aprotinin, Tranexaemic acid & EACA ap-TEM Pre rVIIa adminstration Post rVIIa adminstration Shortened CT Increased α angle Increased MCF
- 27. Antiplatelet Therapy Cyclooxygenase 1/ Thromboxane A2 Inhibitors Asprin ADP Receptor inhibitor - Clopidogrel GP II b / III a Inhibitor – Abiciximab & Tirofiban Traditional Turbidimetric Platelet Aggrgometry Labour Intensive, Expensive, Time consuming Expertise to perform and interpret VEPOCD MA / MCF reflects PF & Fibrinogen levels Platelet Mapping With TEG – Arachidonic acid or ADP added PF in presence of antiplatelet therapy
- 28. Where do we Stand? Time honoured lab tests are still routine High precision, specialists research units are shifting to POCDs VEPOCD have made their entry and are here to stay They give opportunity virtual invivo monitoring of Coagulopathy & Intervention Standardization, education and training are needed Good scope for further research Intensivists need patient oriented problem solving workshops Thank you