10. Angles of the Bladder
• Apex - continuous with • 2 Lateral angles where
the obliterated urachus the ureters enter the
bladder
• Neck - most inferior
part, related to the
superior pelvic fascia
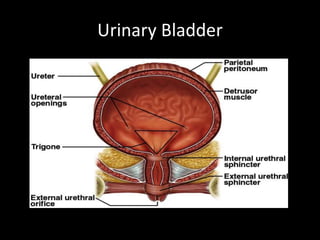
11. Trigone of the Bladder
Triangular area marked by
three openings
Two ureteral orifices
Urethral opening
15. Blood Supply
Vesical arteries
Superior VA
Arises from the proximal part of ant div of Int I A
Divides into numerous br & supply dome of bladder
Middle VA
Br of SVA
Supplies the base of bladder
Inferior VA
Arises from middle rectal or vaginal artery
Base & the Trigone
19. Micturition reflex
Filling of urinary bladder → stretch receptors → sensory
impulse via pelvic nerve to S2 – S4 → Parasympathetic
impulse via pelvic nerve → Contraction of detrusor muscle &
relaxation of internal sphincter → urine in urethra stimulates
stretch receptors → sensory impulse via pelvic nerve to S2 –
S4 → inhibition of somatic fibers in pudendal nerve →
relaxation of external sphincter → results in urination
20. Micturition reflex
Sympathetic (through hypogastric nerve)
stimulation of beta receptors on detrusor muscle
causes relaxation & of alpha receptors on internal
sphincter causes constriction of sphincter, hence
sympathetic stimulation causes filling & referred to
as nerve of filling.
21. Higher brain centers of Micturition
• Facilitatory & inhibitory centers in brain stem
especially pons
• Centers located in cerebral cortex is normally
inhibitory but can become excitatory
• For voluntary urination, cortical centers can
facilitate the sacral micturition centers to help
initiate a micturition reflex & at the same time
inhibit the external urinary sphincter.
22. Voluntary Control of Micturition
• Micturition center in pons receives stretch signals and
integrates cortical input (voluntary control)
• Sends signal for stimulation of detrussor and relaxes internal
urethral sphincter
• To delay urination impulses sent through pudendal nerve to
external urethral sphincter keep it contracted until you wish
to urinate
• Valsalva maneuver
– aids in expulsion of urine by pressure on bladder
– can also activate micturition reflex voluntarily
25. Mechanism of
Bladder injury
Perforation of bladder dome during
Veress needle/trocar insertion
Incidental cystotomy during
development of bladder flap & VVS
in routine/radical Hysterectomy
Adhesiolysis or dissection with
endoscopic scissors with or
without electrosurgery
28. Diagnosis of bladder injuries
Unlike ureteral injuries,
almost all the bladder
injuries are diagnosed
intra-operatively
29. Signs of intra-operative
bladder injuries
• Visualization of the Foley catheter bulb
• Distention of urine collection bag with CO2 (Pneumaturia)
• Urine drainage from accessory trocar site
• Intraperitoneal leakage of Methylene Blue
• Haematuria
• Suprapubic bruising
• Abdominal wall or pelvic mass
• Cystoscopy – size & location
31. Post-operative identification of Bladder injury
Bladder injury is suspected in the presence of:
• Haematuria
• Leakage of urine per vagina ( fistula)
• Fever, flank pain, ileus, abdominal distension
• Sepsis
32. Post-operative
Diagnosis
Cystoscopy
POST-OPERATIVE
VVF
Cystogram
Pad test
IVP
Diagnostic laparoscopy
Cystogram showing VVF
33. Sequelae of Undiagnosed Injuries
• Voiding dysfunction
• Detrusor instability
• Bladder stone formation with recurrent UTI
• Uro-genital fistula formation
• Renal damage
34. Management
Intra-operative bladder injury
Depends on :
Size & location
• Small cystotomy (<10 mm) - Closure followed by
drainage for 5-7 days
• Larger injuries - Laparoscopic or open repair
35. Laparoscopic Bladder injury repair
Cystoscopy
- Exclude injury to trigone
- Check proximity of the defect to the ureter
Remove necrotic tissue, adhesions or areas of
endometriosis before actual repair
37. Laparoscopic Bladder suturing
• Interrupted or continuous absorbable sutures through full
thickness of bladder wall
• Polyglactin or Polydioxanone , no 3-0
• Single layer closure is sufficient
• Repair should include mucosa, muscularis & serosa
• Peritoneal imbrication or omental graft placement between
suture lines may decrease risk of fistula formation
38. Post-operative Period
Bladder drainage with large caliber urethral or
suprapubic catheter
5-7 days - simple fundal laceration
14 days - closer to trigone or vaginal vault
- significant thermal damage
Retrograde cystogram to confirm healing
39. Vesico-vaginal fistula
• Delayed bladder injury presents as a VVF
• Abnormal connection b/w bladder and vagina
• Seen in first 7-10 days post operatively
41. Demographic variation
Obstetric injuries are most common cause of
VVF in developing countries whereas in developed
countries, gynecological surgical injuries are the
commonest cause of VVF.
42. What causes fistula ?
• Direct trauma
• Tissue devacularisation during dissection
• Inadvertent suture placement
• Infection- > tissue necrosis
• Overdistention of bladder post operatively
43. Risk factors
• Previous surgery
• h/o sepsis
• Endometriosis
• Malignancy
• Adhesions with bladder and uterus or cervix
• Anatomical distortion within pelvis
• Radiation
44. Clinical features
Depend on site and size of fistula
• Vaginal leakage
• Recurrent cystitis
• Pyelonephritis
• Unexplained pyrexia
• Hematuria
• Pain: flank, vaginal or supra pubic
• Abnormal urinary stream
• Irritation of vagina and perineum
• Foul odour
45. Type of fistula
Simple - Tissue healthy, good vaginal access
Complicated – large (> 5cms)
scarring
Impaired access
Involvement of ureteric orifices
49. Investigations
• Dye test
• Cysto urethroscopy
• IVP
• Retrograde pyelogram
• Vaginal fluid collection
to see conc. of urea
• Urine analysis and culture
50. Basic principles for fistulae repair
• Ensure that there is no cellulitis, edema, or
infection at the fistula site prior to closing the
fistula
• Excision of avascular scar tissue
• Wide mobilisation of bladder
• Tension free layer closure of bladder and
vagina
• Good hemostasis with bladder drainage
• Using transplanted blood supply
51. Techniques of repair
• Conservative
• Abdominal approach
• Vaginal approach
• Laparoscopic
• Combined
• Electrocautery
• Fibrin glue
• Using interposition flaps or grafts
53. Vaginal vs abdominal approach
Vaginal Abdominal
• In simple fistula • Inadequate vaginal exposure
• When easy access to • For complicated fistula
anterior vaginal wall • Recurrent fistula
e.g, trigonal fistula • Failure of vaginal repair
• Less morbiditiy • Multiple fistula
• Shorter operative time • Larger fistula
• Minimal blood loss • Associated pelvic pathology
• Quicker recovery • In close proximity to ureter
54. Timings of repair
• If diagnosed within 48 hrs post operatively –
immediate repair
Early repair 1-3 months
Late repair 2-4 months
55. Pre operative care
• Urinary or vaginal infection- treated
• Early attempts to divert urinary stream
• Catheter drainage( spontaneous healing in 7 %)
• Care for perineal skin
56. Flap splitting technique
• Adequate exposure made.
• Fistula tract excised with a scalpel
• The entire tract is dissected
• The layers of the bladder wall and vagina
adequately delineated and mobilized
• The bladder mucosa closed with interrupted 4-0
synthetic absorbable suture
• A second layer, the bladder muscle, is closed with
2-0 synthetic absorbable suture.
59. Flap splitting technique
• Vaginal incision closed separately
• The bulbocavernosus muscle transplant ±
• The bladder filled with 200 mL of methylene
blue to ascertain fistula closure.
• Catheter for 3 wks
60. Latzko’s repair
Prerequisites
- Adequate preoperative vaginal vault length
- Fistula located at vaginal apex
Success rate - 89% at first attempt
61. Latzko’s repair
• Obliterates upper vagina for 2-3 cm around the
fistula ( partial colpocleisis)
• An elliptical portion of vaginal epithelium is
stripped in all directions around fistula tract
• Pubovesical fascia closed in two layers
• Vaginal epithelium closed in interrupted sutures
• Posterior vaginal wall becomes the posterior
bladder wall
69. Complications of Fistula Repair
• Post Operative Failure
• Recurrent Fistula Formation
• Injury to Ureter, Bowel, or Intestines
• Vaginal Shortening
70. Prevention of bladder injuries
• Routine drainage of bladder prior to trocar insertion
• Identify the boundaries of the bladder (fill with 200-300 ml NS)
• Meticulous & careful sharp dissection in the presence of
• adhesion, endometriosis or previous LSCS
• Be careful with the use of cautery & while suturing the vault
• Be intrafascial in approach
CYSTOSCOPY at the end
In O’Connors technique, bladder is bi-valved but in modified approach, bi-valving is avoided and and repair is done by making a small incision on the posterior aspect to reachupto the fistula.