
Empfohlen
Empfohlen
Weitere ähnliche Inhalte
Was ist angesagt?
Was ist angesagt? (17)
Andere mochten auch
Ähnlich wie Ebm ims
Ähnlich wie Ebm ims (20)
Ebm ims
- 1. Tropical Medicine and International Health volume 8 no 3 pp 251–258 march 2003 Evidence-based treatment guidelines for sexually transmitted infections developed with and for female sex workers Frieda M. T. F. Behets1,2, Justin Ranjalahy Rasolofomanana3, Kathleen Van Damme1,4, Georgine Vaovola5, Jocelyne Andriamiadana6, Adeline Ranaivo3, Kristi McClamroch2, Gina Dallabetta4, Johannes van Dam 7, Desire Rasamilalao3, Andry Rasamindra and the Mad-STI Working Group* ´ ´ 1 Department of Medicine, School of Public Health, University of North Carolina at Chapel Hill, USA 2 Department of Epidemiology, School of Public Health, University of North Carolina at Chapel Hill, USA 3 Ministry of Health, Antananarivo, Madagascar 4 Family Health International, Research Triangle Park, NC, USA 5 FIVMATA, Diego-Suarez, Madagascar 6 USAID, Antananarivo, Madagascar 7 Population Council, Washington, DC, USA Summary background Sex work is frequently one of the few options women in low-income countries have to generate income for themselves and their families. Treating and preventing sexually transmitted infections (STIs) among sex workers (SWs) is critical to protect the health of the women and their communities; it is also a cost-effective way to slow the spread of HIV. Outside occasional research settings however, SWs in low-income countries rarely have access to effective STI diagnosis. objectives To develop adequate, affordable, and acceptable STI control strategies for SWs. methods In collaboration with SWs we evaluated STIs and associated demographic, behavioural, and clinical characteristics in SWs living in two cities in Madagascar. Two months post-treatment and counselling, incident STIs and associated factors were determined. Evidence-based STI management guidelines were developed with SW representatives. results At baseline, two of 986 SWs were HIV(+); 77.5% of the SWs in Antananarivo and 73.5% in Tamatave had at least one curable STI. Two months post-treatment, 64.9% of 458 SWs in Antananarivo and 57.4% of 481 women in Tamatave had at least one STI. The selected guidelines include speculum exams; syphilis treatment based on serologic screening; presumptive treatment for gonorrhoea, chla- mydia, and trichomoniasis during initial visits, and individual risk-based treatment during 3-monthly follow-up visits. SWs were enthusiastic, productive partners. conclusions A major HIV epidemic can still be averted in Madagascar but effective STI control is needed nationwide. SWs and health professionals valued the participatory research and decision-making process. Similar approaches should be pursued in other resource-poor settings where sex work and STIs are common and appropriate STI diagnostics lacking. keywords sexually transmitted infections, sex workers, risk factors, treatment, prevention, Madagascar, participatory decision-making capital and in port and mining areas. To decrease the STI Introduction burden and to maintain the still relatively low HIV Curable sexually transmitted infections (STIs) are common prevalence, improved primary care of symptomatic STIs in Madagascar (Harms et al. 1994; Behets et al. 1996, has been promoted island-wide, based on research con- 1999, 2001b) and sex work is especially visible in the ducted in Antananarivo in 1997 (Behets et al. 1999, * Amida, Texina Barivelo, Gillian Burkhardt, Rick Homan, Natalie Kruse, Onja Rahamefy, Leonardine Raharimalala, Zo Raharimanana, Jacqueline Rakotoarisoa, Dimisoa Rakotondramarina, Andriamahenina Ramamonjisoa, Jean Rene Randriasamimanana, Norbert ´ Ratsimbazafy, Perle Rasanjimanana, Andry Rasamindrakotroka, Marie Clara Chantal Rasoamanarivo, Andry Rasoloarimanana, Solofoson Rakotonandrasana, Benjamin Ravelojaona, Marie Madeleine Razafinoro, Saholinirina Ranivoarimanana Fleur de Line, Cherif Soliman, Richard Steen. ª 2003 Blackwell Publishing Ltd 251
- 2. Tropical Medicine and International Health volume 8 no 3 pp 251–258 march 2003 F. M. T. F. Behets et al. Management of sexually transmitted infections in sex workers 2001b). STI interventions directed specifically at sex 837 consultations by SWs were recorded during the first workers (SWs) are also needed (Laga et al. 1994) and have 9 months of 1999. In Tamatave, the city with the largest been reported as highly cost-effective to prevent HIV in port, a total of 505 SWs had been registered at the public Africa (Creese et al. 2002). However, effective diagnosis of clinic in November 1999, while in Diego-Suarez, another chlamydial and gonococcal infections in female SWs who port city, 1045 prostitutes were registered through FIV- present for regular follow-up visits requires laboratory MATA, the local SW’s association. SWs in these three cities diagnosis that is not available in most of Madagascar given were encouraged to seek STI care once a month even in its cost, time, personnel, and infrastructure requirements. the absence of any symptoms, but few did; for instance, at In addition, the algorithms that were developed in 1997 for the ‘67 Ha clinic’ only 37% of the consultations by SWs syndromic STI treatment cannot be used for routine were follow-up visits. management of SWs who are most often asymptomatic. The desire to improve STI preventive and curative Prior to 2000, the quality of STI care provided to SWs in services for SWs in Madagascar was shared by a group of Madagascar left much to be desired. For instance, clinical researchers, clinicians, and SWs, and we planned to include exams were not frequently performed and rarely included a SWs as active collaborators throughout the research pelvic exam. SWs were not screened serologically for process. Our research was conducted in three cities in syphilis. Vaginal and occasionally cervical secretions were Madagascar and included three major components: often sub-optimally collected; microscopic exams of the (i) identification of effective and appropriate STI screening genital secretions, interpretation and subsequent manage- and treatment strategies for SWs in Madagascar; (ii) eval- ment of the results were frequently inadequate (extracel- uation of the feasibility and acceptability of improving lular Gram negative diplococci recorded as ‘gono (+)’; clue basic STI services for SWs in partnership with the SWs; cells not recognized, treatment for gonococcal infection (iii) development of national STI treatment guidelines for based on positive microscopy, chlamydial infections SWs based on the research data. In this paper, we will only ignored). present data that were used directly for the development of The laboratory tests that were used for follow-up of SWs the national STI treatment guidelines for SWs. in Madagascar were of doubtful utility given their inherent failure to diagnose gonococcal and chlamydial infections Methods accurately. Routine screening of SWs for STIs based on vaginal smear microscopy may even be harmful because Female SWs were encouraged to present at the non- this practice may create a false sense of security and governmental ‘67 Ha Clinic’ in Antananarivo, and at the encourage sexual risk-taking. Local research was, thus, public dispensary in Tamatave, regardless of symptoms, necessary to identify effective and affordable STI screening through community-based outreach by peer educators. At and treatment strategies for female SWs. enrolment, prevalent STIs, bacterial vaginosis and vulvo- Potential STI management strategies for SWs who vaginal candidiasis were assessed as well as risk factors and present for regular follow-up visits include treatment by markers hypothesized to be associated with these condi- aetiology, i.e. based on laboratory diagnosis (Laga et al. tions. Subsequently, incident STIs and associations with 1994); various forms of presumptive treatment (Steen et al. hypothesized risk variables were evaluated. 2000); and treatment based on individual risk assessment Active female SWs, 16 years of age or older and not (Vuylsteke et al. 1993; Germain et al. 1997; Deceuninck pregnant, who presented to the clinic for newly improved, et al. 2000). Improved clinical services for SWs can be user-centred STI care (through peer educator referral or expected to have an impact on the women’s health and on spontaneously) were invited to participate in the study. STI transmission in the community only to the extent that SWs who had given informed consent, who had not been the SWs use those services. In key informant interviews treated at the clinic during the last 3 months, who were with SWs, it became clear that many women were not willing to comply with treatment regimens and willing and satisfied with the care offered in the public clinics. Clinic able to return for the scheduled follow-up visit were records showed that only a small proportion of active SWs eligible for enrolment. All consenting, eligible SWs pre- attended the existing STI care facilities. In Antananarivo, senting consecutively at the clinics were enrolled. the capital of Madagascar, a total of 1612 SWs had been At the initial visit, the SWs were interviewed by a study registered at the Isotry public clinic in October 1999 but clinician using a structured, pre-tested questionnaire in only 180 SWs had attended this clinic since the beginning Malagasy. A venous blood sample was collected for of 1999. At the ‘67 Ha clinic’, a non-governmental syphilis screening (Macro Vue RPR Card Test, Becton facility in Antananarivo that provides community-based Dickinson, Cockeysville, MD), confirmed by Serodia-TPPA education and clinical services to STI patients and SWs, (Fujirebio, Tokio, Japan) and HIV using EIA (Genetic 252 ª 2003 Blackwell Publishing Ltd
- 3. Tropical Medicine and International Health volume 8 no 3 pp 251–258 march 2003 F. M. T. F. Behets et al. Management of sexually transmitted infections in sex workers Systems Peptide EIA HIV1/2, Sanofi, Pasteur, France), confounders for any other covariates still in the model. confirmed by Western blot (Bio Rad Novapath TM HIV 1 Confounding was determined to exist when removal of the Immunoblot, CA). The women were asked to give no more potentially confounding variables changed the odds ratio than 15 ml of initial stream urine. Urine samples were of a risk factor by at least 10%. aliquoted and frozen at )20 °C until shipped on dry ice to Clinical decision models were developed using the the University of North Carolina for evaluation of gono- factors found to be associated with disease outcome in coccal and chlamydial infections using ligase chain reaction multivariate analysis. The sensitivity, specificity, and pre- (Abbott LCx Probe System, Abbott Laboratories, Abbott dictive values of the developed decision models were Park, IL). calculated following standard methodologies (Fletcher Women were clinically examined, and samples were et al. 1988). The national guidelines were developed collected from the posterior fornix using a swab that was during a 3-day workshop in Madagascar by a group of subsequently immersed in a culture medium for Tricho- researchers, local policy makers and clinicians, and SW monas vaginalis (InPouch, BioMed, San Jose, CA). A representatives who had worked as peer educators in second swab from the lateral vaginal walls was rolled onto Antananarivo, Tamatave, and Diego-Suarez. Local re- a slide for Gram staining. Amine odour and pH of the search results were reviewed, international experience vaginal secretions were assessed. Women were counselled presented, and theoretical and practical, including econo- about treatment and prevention and treated presumptively mic elements of decision-making discussed. Subsequently, with 1 gm of azithromycin and 500 mg of ciprofloxacine, the participants were divided into three working groups. as cervical infections could not be diagnosed effectively Two working groups developed independently STI treat- locally. Additional treatment for trichomoniasis, bacterial ment and prevention guidelines from the perspective of the vaginosis, or reactive syphilis serology was given 1 week care providers and policy makers, and the third working later based on local laboratory results. group formulated guidelines from the perspective of the The follow-up visit, 2 months later, was similar to the users. The final national guidelines, based on research initial visit; the questionnaire concentrated on symptoms results, practical considerations, and local experience and and risk behaviours during the period since the preceding perspectives, were developed by consensus in a plenary visit. All clinical and laboratory evaluations performed at session. the first visit were repeated. The data from the questionnaires, laboratory and clinical Ethical review record forms were entered twice into a database and cleaned using EpiInfo 6.04. Data were analysed using SAS The study was approved by the Committee on the V8 (SAS Institute, Cary, NC). The prevalence and inci- Protection of the Rights of Human Subjects of the dence of bacterial vaginosis, candidiasis, trichomoniasis, University of North Carolina and by the ethical review cervical gonococcal and chlamydial infections were deter- board of the Malagasy Ministry of Health. mined based on laboratory diagnosis. Characteristics hypothesized to be associated with prevalent and incident Results conditions, respectively, were examined using Cochran- Mantel-Haenszel chi-square test or Fisher’s exact test for A total of 986 female SWs (493 in each city) were categorical variables; t-test or analysis of variance for evaluated at the first visit. The median age of the SWs continuous variables. Depending on the probability distri- was 26 years (range 16–57); the median age at which butions of the variables the Wilcoxon rank sum test or the they had started sex work was 21 years (range 11–43). Kruskal–Wallis test were used. While these characteristics did not differ by city, other Independent variables hypothesized to be associated features did and we analysed the data for each city with the outcome of interest were entered into a logistic separately. regression model regardless of the bivariate analyses (Sun Only one woman in each city was found to have HIV et al. 1996). Variables were entered into the model in antibodies at the recruitment visit, but 77.5% of the SWs in groups: behavioural, socio-demographic, and clinical/ Antananarivo and 73.5% of the women in Tamatave had laboratory. The sequence of covariate removal from the at least one curable STI (Table 1). Follow-up data were model was determined by likelihood ratio testing to ensure available for 458 (92.9%) of the SWs in Antananarivo and that the covariate that contributed the least to the fit of the 481 (97.6%) in Tamatave. Roughly 2 months after treat- model would be removed first. Variables that did not ment and advice on prevention of STIs, 64.9% of the SWs significantly contribute to the fit of the model were in Antananarivo and 57.4% of the women in Tamatave evaluated one at the time to determine if they acted as had at least one curable STI. ª 2003 Blackwell Publishing Ltd 253
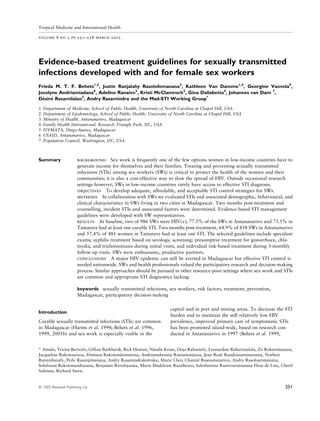
- 4. Tropical Medicine and International Health volume 8 no 3 pp 251–258 march 2003 F. M. T. F. Behets et al. Management of sexually transmitted infections in sex workers Table 1 STIs detected in FSWs in Madagascar at the initial visit and 2 months after presumptive, directly observed therapy Antananarivo, proportion (%) Tamatave, proportion (%) Initial visit Follow-up visit Initial visit Follow-up visit Gonococcal (GC) infection 110/492 (22.4) 84/441 (19.1) 116/483 (24.0) 82/472 (17.4) Chlamydial (CT) infection 83/487 (17.0) 51/442 (11.5) 78/493 (15.8) 32/473 (6.8) GC or CT infection 145/487 (29.8) 101/440 (23.0) 150/484 (31.0) 99/472 (21.0) Trichomoniasis (TV)* 288/493 (58.4) 187/404 (46.3) 220/461 (47.7) 146/480 (30.4) GC, CT or TV* 347/493 (70.4) 220/393 (56.0) 294/471 (62.4) 204/474 (43.0) Syphilis*, 124/491 (25.3) 44/341 (12.9) 164/487 (33.7) 32/315 (10.2) RPR titre 1:8 65/124 (52.4) 12/44 (27.3) 78/164 (47.6) 7/32 (21.9) Any curable STI 382/493 (77.5) 214/330 (64.9) 353/480 (73.5) 225/392 (57.4) Bacterial vaginosis* 290/492 (58.9) 169/380 (44.5) 414/492 (84.2) 390/475 (82.1) Yeast or pseudohyphea* 31/446 (7.0) 43/389 (11.1) 18/492 (3.7) 31/479 (6.5) * Significant difference between Antananarivo and Tamatave, P < 0.05. RPR and TPPA reactive; at follow-up visit results are presented only for women with non-reactive RPR at first visit. Factors associated in logistic regression analysis with Initial visit gonococcal or chlamydial cervical infections detected 2 months after directly observed presumptive therapy are Serologic screening for syphilis using RPR was recom- presented by city in Table 2a and b. Using the beta mended given the documented high prevalence of syphilis coefficients of all the significant predictors in these two in Madagascar, particularly in SWs; the feasibility of this logistic regression models, receiver operator characteristic screening approach if basic resources are made available, (ROC) curves were developed (Figure 1a and b). and the request of the SW representatives to be screened. Confirmatory treponemal testing was not recommended in this context because of its cost and technical complexity. Development of guidelines The service users wanted a speculum exam that allows the The female SWs who participated in the 3-day workshop clinician to detect genital lesions. Presumptive treatment presented their perspective as representatives of the for gonococcal, chlamydial, and trichomonas infections at service users and requested routine serologic screening this initial visit was preferred over selective, risk-based for syphilis and a speculum exam. Of note, while a treatment because of the high prevalence of these STIs. The consensus existed among the health professionals on the recommended frequency of the follow-up visits, i.e. every importance of syphilis screening, the value and feasibility 3 months, was based on the desire of the users, the of speculum exams had been debated. The SW repre- estimated numbers of SWs in the major cities and the sentatives considered a good medical exam essential to capacity of the existing health care facilities. promote patient trust and compliance. The SW repre- sentatives reported that the women want to know what Follow-up visits condition(s) they are suffering from and they considered good communication between the care provider and The technical working group decided that SWs with non- the beneficiary indispensable. Presumptive STI therapy reactive syphilis screening results should be subsequently was deemed acceptable as long as it would be accom- screened using RPR every 3 months. SWs with a reactive panied by explanations given by the clinician and RPR should be screened again 6 months after treatment. preferably also by a peer educator. The SW represent- It was judged that most existing health care facilities cannot atives thought that care including treatment should not currently be expected to perform quantitative RPR testing cost more than 5000 FMG (about 0.77 US$) and that for follow-up. Therefore, and in light of the high preval- consultations should start at 7:30 a.m. Lastly, more peer ence and exposure to syphilis, SWs with a reactive RPR educators should be involved in clinic-based STI care and 6 months after adequate treatment should be treated again prevention for female SWs. The national guidelines with two doses of 2.4 MIU benzathine penicillin given at (Table 3) were subsequently developed by consensus 1-week interval, despite the fact that a sizeable proportion based on the following rationale. of these women may no longer have infectious syphilis. 254 ª 2003 Blackwell Publishing Ltd
- 5. Tropical Medicine and International Health volume 8 no 3 pp 251–258 march 2003 F. M. T. F. Behets et al. Management of sexually transmitted infections in sex workers Table 2 Factors associated with incident cervical infection detected 2 months after Variable OR (95% CI) presumptive therapy in FSWs in (a) Anta- (a) Antananarivo nanarivo (n ¼ 308) and (b) Tamatave Age <25 years 1.55 (0.83, 2.90) (n ¼ 461) At least 10 partners in the past week 4.28 (1.97, 9.29)* Used condom at last sex act 0.31 (0.11, 0.87)* Absence of lactobacilli in vaginal flora 2.89 (0.97, 8.62) Endocervical mucopus 5.02 (1.60, 15.68)* Incident bacterial vaginosis 2.64 (1.33, 5.25)* Prompted report of abnormal vaginal discharge 2.14 (1.11, 4.11)* Confounders Prompted report of vaginal itching or burning 1.70 (0.77, 3.74) Prompted report of bleeding between periods 0.52 (0.08, 3.47) Cervical erosion on exam 0.65 (0.34, 1.25) (b) Tamatave Age <25 years 2.35 (1.41, 3.93)* At least 10 partners in the past week 2.16 (1.05, 4.44)* Reported condom use at last commercial sex act 4.13 (1.49, 11.44)* Education Primary vs. post-primary 2.44 (1.27, 4.71)* Less than primary vs. post-primary 4.97 (2.39, 10.31)* Truck driver client in the past month 2.41 (1.27, 4.57)* Absence of lactobacilli in vaginal flora 7.91 (2.20, 28.40)* Cervical erosion on exam 2.04 (1.14, 3.65)* Cervical friability on exam 2.65 (1.47, 4.77)* Spontaneous complaint of malodorous discharge 0.47 (0.27, 0.83)* Confoundersà Taxi driver client in the past month 0.73 (0.39, 1.38) Used condom at last sex act 2.09 (0.37, 11.80) Prompted report of pain during intercourse 0.38 (0.14, 1.05) * Adjusted odds ratio significantly different from 1, P < 0.05. Includes confounders of variables significantly associated with incident cervical infection. à Confounders of variables significantly associated with incident cervical infection. Vari- ables omitted from the final model because of small numbers: recruited client from ports in the past month and prompted report of bleeding between periods. The decision to treat a SW for trichomoniasis/bacterial workshop. During the decision-making process, the sta- vaginosis in the presence of malodorous vaginal discharge bility of the risk factors for cervical infections with regard or a vaginal pH greater than 4.5 was based on the overall to place, time, and implementer, the acceptability by 95.6% sensitivity (95% CI: 94.1–97.1); the 46.8% specif- stakeholders and environmental constraints as well as the icity (95% CI: 38.9–54.7), and the 88.2% positive cost and the effectiveness of various options were discussed predictive value (95% CI: 85.8–90.6) determined during and made as explicit as possible (Behets et al. 2001a). Age simulation analyses of the empirical research results. The <25 years, at least 10 sex partners during the last week, sensitivity of this approach was 91.5% in Antananarivo vaginal pH >4.5 (or absence of lactobacilli in vaginal (95% CI: 87.9–95.1) and 98.0% in Tamatave (95% CI: smear), and clinical signs of cervicitis or motion tenderness 98.0–98.0); the specificity was 57.8% in Antananarivo were selected as risk factors for the algorithm (Table 3). To (95% CI: 47.2–68.4) and 33.8% in Tamatave (95% CI: avoid the need for systematic microscopic examinations 22.8–44.8); the positive predictive value was 86.1% in and allow the use of a less costly and less demanding Antananarivo (95% CI: 81.8–90.4) and 89.4% in Tama- screening test, vaginal pH >4.5 was substituted for absence tave (95% CI: 86.5–92.3). of lactobacilli. The findings of the multivariate analyses (Table 2) served The ROC curves obtained for the selected algorithm are as the basis to select the algorithm for management of presented in Figure 1a and b. Using a cut-off value of 3, lower genital tract infections due to Neisseria gonorrhoea the sensitivity of the selected algorithm was 83.7% or Chlamydia trachomatis at follow-up visits during the overall (95% CI: 81.2–86.2), 82.6% in Antananarivo ª 2003 Blackwell Publishing Ltd 255
- 6. Tropical Medicine and International Health volume 8 no 3 pp 251–258 march 2003 F. M. T. F. Behets et al. Management of sexually transmitted infections in sex workers 1 There were some differences between the two cities, (a) illustrating the need to conduct this type of research on 0.9 STIs in various settings within one country. We found 0.8 differences in STIs and in associated risk factors between 0.7 the women evaluated in the capital and the women in the Sensitivity 0.6 port city. Cervical infection was associated with lower 0.5 educational levels in Tamatave but not in Antananarivo. 0.4 Interestingly, reported condom use for the last sex act was 0.3 associated with a lower risk for cervical infection in the capital and with a higher risk in Tamatave. While this 0.2 Selected model finding could reflect reporting issues, it could also be due to 0.1 Best model different transmission dynamics as suggested by the fact 0 that sex with a truck driver in the past month was an 1 independent risk factor for incident cervical infection in (b) Tamatave but not in Antananarivo. Most women in this 0.9 study reported that the majority of their recent sex acts 0.8 were not protected by condom use, thus condom use at last 0.7 sex act can be expected to be a poor predictor. Sensitivity 0.6 Despite the differences in risk factors for cervical 0.5 infections by city, a single STI care strategy for SWs in Madagascar was developed that was acceptable to the 0.4 participating health professionals, and to the SWs who 0.3 represented the service users. We opted for presumptive 0.2 treatment of gonococcal and chlamydial infections and Selected model 0.1 Best model trichomoniasis the first time a SW seeks care for STIs while 0 for the 3 monthly follow-up visits these infections are 0.1 0.2 0.3 0.4 0.5 0.6 0.7 0.8 0.9 1 treated based on individual risk assessments. Three 1-Specificity monthly repeat visits with treatment based on the results of a clinical examination and on an assessment of individual Figure 1 Receiver operator characteristics curves for incident risk factors were preferred to periodic presumptive treat- cervical infections in (a) Antananarivo and (b) Tamatave. ments to avoid negative psychological reactions when SWs repeatedly receive the same treatment. It was felt that SWs (95% CI: 78.7–86.5), and 84.7% in Tamatave (95% might become uncertain of the quality of the STI services CI: 81.4–88.0). The specificity of treating cervical infec- and less open to educational messages when clinicians tion in the presence of a risk score of at least 3 was prescribe the same drugs. Similarly, clinicians may become 36.6% overall (95% CI: 33.3–39.9), 30.3% in Antanan- bored and less efficient in counselling to prevent STIs. arivo (95% CI: 25.6–35.0), and 41.2% in Tamatave Interestingly, economic analyses did not show a convincing (95% CI: 36.7–45.7). The positive predictive value of this benefit of periodic presumptive treatment in terms of algorithm was 27.3% overall (95% CI: 24.3–30.3), reducing the STI prevalence (data not shown). 26.9% in Antananarivo (95% CI: 22.3–31.5), and 27.6% Clinical algorithms developed for female SWs in other in Tamatave (95% CI: 23.6–31.6). countries do not distinguish first from follow-up visits (Vuylsteke et al. 1993; Germain et al. 1997; Deceuninck et al. 2000). Simple laboratory tests such as the detection Discussion of intra-cellular Gram-negative diplococci in cervical smear The importance of providing adequate STI care and (Deceuninck et al. 2000) or >10 leucocytes/field in vaginal prevention interventions to SWs in Madagascar was smears (Germain et al. 1997) have been included elsewhere demonstrated by the documented high burdens of disease in algorithms for SWs. The sensitivity of these algorithms and the high exposures to re-infection. While curable STIs ranged from 58% to 71% with specificities from 56% to were an important public health problem in these women, 80%. We selected an algorithm for cervical infections that only two persons were infected with HIV, suggesting that does not require laboratory testing but that includes Madagascar is still in a good position to avoid a disastrous vaginal pH in the risk assessment. This can be measured HIV epidemic. immediately by the clinician and is inexpensive. In our 256 ª 2003 Blackwell Publishing Ltd
- 7. Tropical Medicine and International Health volume 8 no 3 pp 251–258 march 2003 F. M. T. F. Behets et al. Management of sexually transmitted infections in sex workers Table 3 Summary National Guidelines for STI treatment and prevention in female sex workers in Madagascar Initial visit 1. Serologic screening using RPR; treatment for syphilis if RPR-reactive 2. Speculum exam; treatment for syphilis & chancroid if genital ulcers present* 3. Presumptive treatment of gonococcal and chlamydial infection, and trichomoniasis/bacterial vaginosis (BV) 4. Promotion of condom use, counselling, and invitation for follow-up visit 3 months later Follow-up visit 1. Serologic screening using RPR if last result non-reactive or obtained at least 6 months earlier; treatment for syphilis if RPR-reactive 2. Speculum exam; treatment for syphilis and chancroid if genital ulcers present* 3. Risk-based treatment 3.1. Trichomoniasis/BV if malodorous discharge or vaginal pH > 4.5 3.2. Candidiasis if genital itching or burning or woman pregnant 3.3. Gonococcal and chlamydial infection if total risk score at least 3 Risk factor (score) Age <25 years (1) At least 10 partners in last week (1) Vaginal pH > 4.5 (or absence of lactobacilli) (2) Any sign of cervicitis or motion tenderness (1) 4. Promotion of condom use, counselling, and invitation for follow-up visit 3 months later * Treat and counsel for HSV when lesions are recurrent and vesicular. Endocervical mucopus or cervical friability or cervical erosion. experience, even simple microscopy can be a strain on researchers. Including laypersons with little formal educa- human and logistical resources in settings with few tion in decision-making entailed challenges and risks due to resources and the quality is usually highly dependent on limited or inadequate understanding of technical aspects location or staff and may vary over time. We selected a few and concepts. During the course of the field research, the risk factors for clinical management that were judged most SW representatives had acquired basic notions of STI care practical and stable across geographic locations, health and prevention. We made efforts to explain in plain care settings, and over time. As shown by the ROC curves, language concepts such as antimicrobial resistance, pre- even the best models obtained by logistic regression dictive values, and misclassification costs. However, the performed modestly and did not differ much from the SW representatives could not be expected to have the same selected algorithm for management of cervical infection. grasp of the technical issues as the health professionals. We Our algorithm, like all clinical algorithms based on risk debated the pros and cons of including SW representatives assessment, will need periodic re-evaluations since STI in each of the three working groups at the decision-making prevalence and associated risk factors will evolve, partic- workshop vs. creating one separate working group con- ularly in settings with active prevention programmes. stituted of peer educators only. We opted for the latter to To develop these national STI management guidelines enable a more independent voice of the users despite the for female SWs, we followed a decision-making process risk of discrepant and possibly irreconcilable opinions and that was similar to the one we used in 1997 when the demands. Fortunately, the conclusions presented by the national STI treatment algorithms for symptomatic three working groups at the plenary session showed few patients were developed. While researchers, public health and manageable differences and a consensus was reached. workers as well as public and private sector clinicians were The research project was conceived with an explicit involved in the decision-making process in 1997, patient desire to promote empowerment of SWs and their organ- representatives were not. The inclusion of peer educators in izations. The active engagement of the peer educators in 2001 offered opportunities to better understand and the research and in the decision-making workshop was a integrate user perspectives that might ultimately improve positive experience; the peer educators enthusiastically acceptability to and use of STI services by SWs. endorsed the opportunity to contribute actively to decision- We believed that participatory action research (Minkler making and health professionals had the opportunity to 2000) was necessary to improve STI care and prevention understand more effectively the experiences, outlooks, for SWs in Madagascar. Actively involving SWs through- concerns, and needs of the SWs. However, empowerment out the research was a learning process for SWs and of SWs in this project was confined to a predominantly ª 2003 Blackwell Publishing Ltd 257
- 8. Tropical Medicine and International Health volume 8 no 3 pp 251–258 march 2003 F. M. T. F. Behets et al. Management of sexually transmitted infections in sex workers biomedical intervention and can only be considered as one Deceuninck G, Asamoah-Adu C, Khonde N et al. (2000) step towards better life conditions and improved economic Improvement of clinical algorithms for the diagnosis of Neis- options for these women. seria gonorrhoeae and Chlamydia trachomatis by the use of Gram-stained smears among female sex workers in Accra, Ghana. Sexually Transmitted Diseases 27, 401–410. Acknowledgement Fletcher RH, Fletcher SW & Wagner EH (1988) Clinical Epide- miology, 2nd edn. Williams & Wilkins, Baltimore. We are grateful for critical support from Wendy Githens Germain M, Alary M, Guedeme A et al. (1997) Evaluation of a Benazerga. screening algorithm for the diagnosis of genital infections with Neisseria gonorrhoeae and Chlamydia trachomatis among female sex workers in Benin. Sexually Transmitted Diseases 24, References 109–115. Behets FMT, Andriamahenina R, Andriamiadana J, May JF & Harms G, Kirsch T, Rahelimiarana N et al. (1994) HIV and Rasamindrakotroka A (1996) High syphilis and low but rising syphilis in Madagascar. Aids 8, 279–280. HIV seroprevalence rates in Madagascar. Lancet 347, 831. Laga M, Alary M, Nzila N et al. (1994) Condom promotion, Behets FMT, Andriamiadana J, Randrianasolo D et al. (1999) sexually transmitted diseases treatment, and declining incidence Chancroid, primary syphilis, genital herpes, and lymphogranu- of HIV-1 infection in female Zairian sex workers. Lancet 344, loma venereum in Antananarivo, Madagascar. Journal of 246–248. Infectious Diseases 180, 1382–1385. Minkler M (2000) Using participatory action research to build Behets FM, Miller WC & Cohen MS (2001a) Syndromic treatment healthy communities. Public Health Reports 115, 191–197. of gonococcal and chlamydial infections in women seeking Steen R, Vuylsteke B, DeCoito T et al. (2000) Evidence of decli- primary care for the genital discharge syndrome: decision- ning STD prevalence in a South African mining community making. Bulletin of the World Health Organization 79, following a core-group intervention. Sexually Transmitted 1070–1075. Diseases 27, 1–8. Behets F, Andriamiadana J, Rasamilalao D et al. (2001b) Sexually Sun GW, Shook TL & Kay GL (1996) Inappropriate use of transmitted infections and associated socio-demographic and bivariable analysis to screen risk factors for use in multivariable behavioural factors in women seeking primary care suggest analysis. Journal of Clinical Epidemiology 49, 907–916. Madagascar’s vulnerability to rapid HIV spread. Tropical Vuylsteke B, Laga M, Alary M et al. (1993) Clinical algorithms for Medicine and International Health 6, 202–211. the screening of women for gonococcal and chlamydial infec- Creese A, Floyd K, Alban A & Guinness L (2002) Cost-effective- tion: evaluation of pregnant women and prostitutes in Zaire. ness of HIV-AIDS interventions in Africa: a systematic review of Clinical Infectious Diseases 17, 82–88. the evidence. Lancet 359, 1635–1642. Authors Dr Jocelyne Andriamiadana, USAID, Antananarivo, Madagascar. E-mail: sandriamiadana@usaid.gov Dr Frieda M.-T. F. Behets, School of Public Health, University of North Carolina at Chapel Hill, 2102A McGavran-Greenberg Hall, CB 7435, Chapel Hill, NC 27599-7400, USA. Tel.: +1 919 966 7440; Fax: +1 919 966 2089; E-mail: frieda_behets@unc.edu (corresponding author). Dr Gina Dallabetta, Family Health International, Research Triangle Park, NC, USA. E-mail: gdallabetta@fhi.org Kristi McClamroch, Department of Epidemiology, School of Public Health, University of North Carolina at Chapel Hill, 2102A McGavran-Greenberg Hall, CB 7435, Chapel Hill, NC 27599-7400, USA. Dr Adeline Ranaivo, Ministry of Health, Antananarivo, Madagascar. Dr Justin Ranjalahy Rasolofomanana, Institut National de sante dublique et communautaire, 74 Rue du 26 Suin 1960, Antananarivo, ´ Madagascar. E-mail: inspc-directeur@iris.mg Dr Desire Rasamilalao, Ministry of Health, Antananarivo, Madagascar. ´ ´ Dr Johannes van Dam, Population Council, Washington, DC, USA. E-mail: jvandam@pcdc.org Dr Kathleen Van Damme, Family Health International, Research Triangle Park, NC, USA. E-mail: kvandamme@dts.mg Georgine Vaovola, FIVMATA, Diego-Suarez, Madagascar. Dr Andry Rasamindkakotroka, E-mail: arasamin@syfed.refer.mg 258 ª 2003 Blackwell Publishing Ltd