Septic shock
•Als PPT, PDF herunterladen•
33 gefällt mir•4,724 views

Lecture องค์กรแพทย์ เรื่องติดเชื้อในกระแสเลือด Septic Shock

Empfohlen
Weitere ähnliche Inhalte
Was ist angesagt?
Was ist angesagt? (20)
Andere mochten auch
Andere mochten auch (20)
Ähnlich wie Septic shock
Ähnlich wie Septic shock (20)
Mehr von ปิติ นิยมศิริวนิช
Mehr von ปิติ นิยมศิริวนิช (10)
Kürzlich hochgeladen
Kürzlich hochgeladen (20)
Septic shock
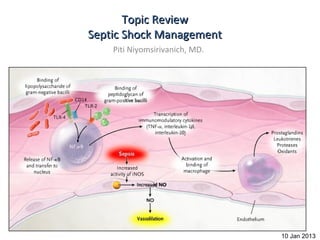
- 1. Topic Review Septic Shock Management Piti Niyomsirivanich, MD. 10 Jan 2013
- 2. Take home message • Adequate preload • Appropriate Antibiotic within 1 hr • Proper dose of vasopressors • Consult
- 3. Outline • Definition • Pathophysiology • Early Goal Directed Therapy • Fluid Resuscitation • Vasopressors • Steroids • Antibiotics • Glucose control • Blood product administration • Bicarbonate therapy • Stress ulcer prophylaxis
- 4. Definition • Bacteremia : Bacteria in blood • Septicemia : Bacteria + toxin in blood • SIRS : 2/4 of following conditions – 1)Temp > 38 C or < 36 C – 2) Pulse rate > 90 /min – 3) RR > 20 /min or PaCO2 < 32 mmHg – 4) WBC > 12,000/ul or < 4000 /ul and/or Band form > 10% • Sepsis = SIRS from infection • Severe sepsis = Sepsis+ end organ damage – CVS , Renal , pulmonary , Hematologic ,Metabolic acidosis • Septic Shock = Sepsis + hypotension
- 6. Guideline Surviving Sepsis Campaign: International guidelines for management of severe sepsis and septic shock:2008
- 7. Since 2001 10+ years ago!!!
- 9. Result of EGDT N Engl J Med 2001; 345:1368- 1377 November 8, 2001
- 10. Early goal directed therapy SIRS + SBP < 90 mmHg or MAP < 65 mmHg ONE -Or- Lactate > 4 mmol/L Hour After 20-30 ml/kg crystalloid IVF Culture Supplement oxygen Antibiotic within 1 hour Critical care consultation or ET tube (if necessary) Volume accessment < 8-12 mmHg CVP ? IVF 8-12 mmHg < 65 mmHg Five MAP ? Vasopressor (NE/dopamine) Hours >/= 65 mmHg < 70% Blood transfusion to Hct > 30% ScvO2 ? > 70% Inotropic agent Goals achieved Sedatives & muscle relaxants Resuscitation complete N Engl J Med 2001; 345:1368-1377November 8, 2001
- 12. Fluid Resusitation • Fluid therapy – crystalloids or colloids (1B) – Target a CVP of 8-12 mmHg (1C) – Give fluid challenges of 1000 mL of crystalloids • or 300–500 mL of colloids over 30 mins. Surviving Sepsis Campaign: International guidelines for management of severe sepsis and septic shock:2008
- 14. Shock • BP = CO X TVR • CO = HR X SV • SV = EDV – ESV • BP = ( EDV- ESV ) X HR X TVR X EDV EDV • BP = EF X HR X TVR X EDV
- 15. Volume N Engl J Med 2001; 345:1368- 1377November 8, 2001
- 17. Fluid • Crystalloids – NSS – Ringer Lactate Solution • Colloids – albumin – Dextrans – Gelatins e.g. Haemaccel – Hydroxyethylstarch e.g. Voluven
- 18. Fluid • Crystalloids – NSS Low cost – Ringer Lactate Solution edema • Colloids Hemodilution Hyperchloremic metabolic acidosis – albumin – Dextrans – Gelatins e.g. Haemaccel – Hydroxyethylstarch e.g. Voluven
- 19. Fluid • Crystalloids – NSS Low cost – Ringer Lactate Solution Lactate liver Acetate peripheral tissue • Colloids Potassium – albumin edema – Dextrans – Gelatins e.g. Haemaccel – Hydroxyethylstarch e.g. Voluven
- 20. Fluid • Crystalloids – NSS SAFE Study * – Ringer Lactate Solution not differrent VS NSS • Colloids hypocalcemia – albumin expensive – Dextrans – Gelatins e.g. Haemaccel – Hydroxyethylstarch e.g. Voluven *A Comparison of Albumin and Saline for Fluid Resuscitation in the Intensive Care Unit N ENGL J MED 2004; 350:2247-2256 May 27, 2004
- 21. Fluid • Crystalloids Coagulopathy (inh. F VIII/ vWF) – NSS Renal damage – Ringer Lactate Solution Cross matching problem • Colloids Osmotic diuresis – albumin Anaphylaxis 0.27% – Dextrans – Gelatins e.g. Haemaccel – Hydroxyethylstarch e.g. Voluven
- 22. Fluid • Crystalloids Gelofundol Haemaccel – NSS – Ringer Lactate Solution 30,000-35,000 kDa • Colloids Renal Excretion – albumin Short half life – Dextrans Anaphylaxis 0.34% – Gelatins e.g. Haemaccel – Hydroxyethylstarch e.g. Voluven
- 23. Fluid • Crystalloids • MW 450-480 kDa Hetastarch Hespan – NSS •MW 200 kDa – Ringer Lactate Solution •HAES-Steril 6%,10% • Colloids •MW 70 kDa •HES 70/0.5 – albumin •Voluven – Dextrans Anaphylaxis 0.058% – Gelatins e.g. Haemaccel – Hydroxyethylstarch e.g. Voluven
- 24. Cochrane Database Syst. Rev. CD 001319,2003
- 25. Volume Assessment • Static VS dynamic • Non-invasive – U/S IVC – Passive leg raising test – Pulse oximetry plethysmographic waveform amplitude variation • Invasive – CVP – Fluid challenge test – CVP variation – Pulse pressure variation
- 26. Volume Assessment • Require Endotracheal tube • No Endotracheal tube • W/WO Endotracheal tube
- 27. CVP measurement a= Atrial contraction c= Ventricular Contraction x= Atrial relaXation v= Venous filling y = Tr”Y”cuspids opening
- 28. CVP • CVP : poor predictor of fluid volume CHEST. July 2008;134(1):172-178.
- 29. Fluid Challenge Test for CVP Load IV fluid 200-250 ml in 10 min CVP + CVP + CVP + </=2 2-5 >/=5 Continue fluid therapy Wait Decrease rate of fluid therapy
- 30. Ultrasound IVC Caval Index = 100 x (diam expiration - diam inspiration)/diam expiration Caval Index > 50% suggest low CVP Ann Emerg Med 2010; 55:290-295.
- 31. Passive leg raising test Esophageal doppler : in cardiac output > 8% predict fluid responsiveness Critical Care 2006, 10:170
- 32. Pulse oximetry plethysmographic waveform amplitude variation
- 33. CASE A CASE B CVP =15 cmH2O CVP =5 cmH2O
- 34. Pulse oximetry plethysmographic waveform amplitude variation %POP variation POP max – POP min X 100 > 13% POP mean
- 35. Arterial Line
- 37. Vasopressor therapy • Dopamine VS Norepinephrine Kaplan–Meier Curves for 28-Day Survival in the Intention-to-Treat Population. N Engl J Med 2010; 362:779-789
- 38. Vasopressure therapy Dopamine Low dose Moderate dose (beta adrenergic receptor ) 5-10 ug/kg/min High dose (alpha adrenergic receptor) >10 ug/kg/min Maximum dose 50 ug/kg/min Norepinephrine start 0.5 mcg/min Harrison Int. Med edition 18 th
- 39. Vasopressor therapy Example ผู้หญิง 64 ปี หนัก 70 kg มาด้วย ไข้ หนาวสั่น ปัสสาวะแสบขัด CBC : WBC 25000/ul N% 85 Band 2% Hb 12 g/dl Plt 200,000/ul UA WBC 50-100 BP 80/40 mmHg PR 95/min Temp 37.8 C RR 18/min จงคำานวณ dose ของ Dopamine ให้ start 5 ug/kg/min
- 40. Vasopressor therapy Example ผู้หญิง 64 ปี หนัก 70 kg มาด้วย ไข้ หนาวสัน ปัสสาวะแสบขัด ่ CBC : WBC 25000/ul N% 85 Band 2% Hb 12 g/dl Plt 200,000/ul UA WBC 50-100 BP 80/40 mmHg PR 65/min Temp 37.8 C RR 18/min จงคำานวณ dose ของ Dopamine ให้ start 5 ug/kg/min 60 X W (kg) X D (ug/kg/min) Rate (ml/min) C Solute C= 1,000 Volume
- 41. Vasopressor therapy Example ผู้หญิง 64 ปี หนัก 70 kg มาด้วย ไข้ หนาวสัน ปัสสาวะแสบขัด ่ CBC : WBC 25000/ul N% 85 Band 2% Hb 12 g/dl Plt 200,000/ul UA WBC 50-100 BP 80/40 mmHg PR 65/min Temp 37.8 C RR 18/min จงคำานวณ dose ของ Dopamine ให้ start 5 ug/kg/min 60 X 70 X 5 Rate (ml/min) = 10.5 ml/hr 2000 1000 C= 1,000 = 2000 500 (Dopamine 1000 mg ผสม 5%D/W 500 ml)
- 42. Early goal directed therapy SIRS + SBP < 90 mmHg or MAP < 65 mmHg ONE -Or- Lactate > 4 mmol/L Hour After 20-30 ml/kg crystalloid IVF Culture Supplement oxygen Antibiotic within 1 hour Critical care consultation or ET tube (if necessary) Volume accessment < 8-12 mmHg CVP ? IVF 8-12 mmHg < 65 mmHg Five MAP Vasopressor (NE/dopamine) Hours >/= 65 mmHg < 70% Blood transfusion to Hct > 30% ScvO2 > 70% Inotropic agent Goals achieved Sedatives & muscle relaxants Resuscitation complete N Engl J Med 2001; 345:1368-1377November 8, 2001
- 43. ScvO2 ให้เงินไป โรงเรียน ขากลับ เหลือ 50 บาท แปลว่าให้เงินไปโรงเรียนพอใช้
- 44. ScvO2 O2 content O2 content เหลือ 70% แปลว่าให้ออกซิเจนไปเนือเยือพอใช้ ้ ่
- 45. ScvO2
- 46. O2 delivery • DO2 = [1.39 x Hb x SaO2 + (0.003 x PaO2)] x CO • Depend on < 70% Blood transfusion to Hct > 30 ScvO2 – Hemoglobin > 70% Inotropic agent – O2 saturation Goals achieved – Cardiac output – ScvO2 < 70% • target Hct > 30 • Inotropic drug increase cardiac output Contin Educ Anaesth Crit Care Pain (2004) 4 (4) 123-126
- 47. Alternative for ScvO2 • Lactate clearance – lactate clearance >10% or higher • 6% lower in-hospital mortality than those resuscitated to an ScvO2 of at least 70% – (95% CI, −3% to 15%) – noninferiority trial. JAMA. 2010 Feb 24;303(8):739-46.
- 48. Antimicrobial Therapy • administration of broad-spectrum antibiotic therapy within 1 hr of diagnosis of septic shock (1B) and severe sepsis without septic shock (1D); • reassessment of antibiotic therapy with microbiology and clinical data to narrow coverage, when appropriate (1C); • a usual 7–10 days of antibiotic therapy guided by clinical response (1D); • source control with attention to the balance of risks and benefits of the chosen method (1C); Survival Sepsis Guideline .Crit Care Med 2008
- 49. Empirical Antibiotic • Host – Immunocompetent – Neutropenia – IVDU – Post Splenectomy – AIDS • Risk factors & exposures • Site of infection • Antibiotics of choice ?? Antibiotic therapy in patients with septic shock European Journal of Anaesthesiology (EJA). 28(5):318-324, May 2011
- 50. Tips • every 10 min, survival is decreased by 1%.* • First dose Full dose – Then renal adjustment * Antibiotic therapy in patients with septic shock European Journal of Anaesthesiology (EJA). 28(5):318-324, May 2011
- 51. De-escalate Therapy • De-escalate Empirical antimicrobial therapy in life-threatening situations – Start with Broad Spectrum • ‘Broad-spectrum antibiotics’ refers to antibiotics with activity against Pseudomonas aeruginosa, including imipenem-cilastatin, piperacillin-tazobactam, ceftazidime or ciprofloxacin. • Limited-spectrum antibiotics will only refer to β-lactam antibiotics without activity against P. aeruginosa (essentially, ceftriaxone and amoxicillin-clavulanate). Antibiotic therapy in patients with septic shock European Journal of Anaesthesiology (EJA). 28(5):318-324, May 2011
- 52. De-escalate Therapy : Life Threatening • "สันๆ แต่ aggressive" แล้วปรับลงมา ้ – Recurrent infections were more common in Group No De-escalate (19% versus 5%, P = 0.01) – An inadequate empiric antibiotic therapy was more frequent in Group No De-escalate (27.5% versus 7.7% P = 0.02) – Mortality between the two groups 18.3% (D) vs 24.6% (ND) Critical Care 2010, 14:R225
- 53. Antibiotic therapy in patients with septic shock European Journal of Anaesthesiology (EJA). 28(5):318-324, May 2011
- 55. Steroids in CIRCI (critical illness related corticosteroid insufficiency) •stress-dose steroid therapy given only in septic shock after blood pressure is identified to be poorly responsive to fluid and vasopressor therapy (2C) •Survival Sepsis Guideline 2008 Serum cortisol •< 15 ug/dl definite adrenal insufficiency •13-35 ug/dl Suspected •>35 ug/dl no benefit •สมาคมเวชบำาบัดวิกฤติแห่งประเทศไทย
- 56. Steroids in CIRCI Surge in cortisol (> 9 ug/dl) response to ACTH 250 ug stimulation Benefit from steroids JAMA. 2002 Aug 21;288(7):862-71
- 57. CIRCI Baseline cortisol level < or = 35 microg/dl is a useful diagnostic threshold for diagnosis of steroid responsiveness in Thai patients with septic shock ACTH stimulation test should not be used sensitivity was 85%, the specificity was 62% J Med Assoc Thai 2010 Jan;93 Suppl 1:S187-95
- 58. CIRCI • Hydrocortisone 100 mg bolus then 200 mg V drip in 24 hr • OR • Hydrocortisone bolus q 4-6 hr NOT q 8 hr – e.g. Hydrocortisone 50 mg V q 6 hr • Then taper off
- 60. Blood Sugar control • NICE-SUGAR study – 3050 patients – Medicine & Surgery Ward – Multicenter randomized open label study – ICU & non ICU – Intensive control 81-108 mg% – Conventional control 144-180 mg% The NICE-SUGAR Study Investigators N Engl J Med 2009; 360:1283-1297March 26, 2009
- 61. NICE-SUGAR Study The NICE-SUGAR Study Investigators N Engl J Med 2009; 360:1283-1297March 26, 2009
- 65. Basal Insulin with Scheduled Insulin (prandial insulin) with Correctional dose
- 67. • CBG (ก่อนอาหาร) เช้า กลางวัน เย็น ก่อนนอน
- 68. Somchai Pathanaangkul ,Royal Thai Army Medica Vol 57 No.4 Oct.-Dec. 2004
- 69. Blood Transfusion ● Give red blood cells when hemoglobin decreases to 7.0 g/dL (70 g/L) to target a hemoglobin of 7.0–9.0 g/dL in adults (1B). A higher hemoglobin lev el may be required in special circumstances (e.g., myocardial ischaemia, se vere hypoxemia, acute hemorrhage, cyanotic heart disease, or lactic acidosi s) ● Do not use erythropoietin to treat sepsis-related anemia. Erythropoietin may be used for other accepted reasons (1B) Do not use fresh frozen plasma to correct laboratory clotting abnormalities unless there is bleeding or planned i nvasive procedures (2D) ● Do not use antithrombin therapy (1B) Administer platelets when (2D) Counts are 5000/mm3 (5 109/L) regardless of bleeding Counts are 5000–30,000/mm3 (5–30 109/L) and there is significant bleeding risk Higher platelet counts (50,000/mm3 [50 109/L]) are required for surgery or invasive procedures
- 70. Blood Transfusion • TRICC Study – Study design: Multicenter RCT – Setting: 25 ICUs across Canada – Hb • 7-9 g/dl (Restrictive Strategy) • 10-12 g/dl (Liberal Strategy) – Primary Outcome : mortality rate 30 days – Results • Hb 7-9 g/dl group mortality rate 22.2% • Hb 10-12 g/dl mortality rate 28.1% • (P=0.05)
- 71. TRICC Study Hb 7-9 g/dl Hb 10-12 g/dl
- 72. Bicarbonate Therapy • We recommend against the use of sodium bicarbonate therapy for the purpost of improving hemodynamics or reducing vasopressure requirement with hypoperfusion-induced lactic acidemia with pH > 7.15 (1B) Surviving Sepsis Campaign: International guidelines for management of severe sepsis and septic shock:2008
- 73. Hb O2 Dissociation curve
- 74. Stress Ulcer Prophylaxis • We recommend that stress ulcer prophylaxis using H2 blocker (1A) • Or PPI (1B) be given to patients with severe sepsis to prevent upper GI bleed. • Weighted aginst the potential effect of an increased stomach pH on development of VAP Surviving Sepsis Campaign: International guidelines for management of severe sepsis and septic shock:2008
- 75. Other • Sucralfate* – Not associated with an increase in stress ulceration. – Less impact gastric colonization Less VAP – Increase aspiration • Enteral Feeding *EAST Practice Management Guidelines Committee
- 76. Take home message • Adequate preload • Antibiotic within 1 hr • Proper dose of vasopressors. • Consult
- 77. Thank you