3. ANATOMYANATOMY
The tonsils are 3 masses of tissue:
- lingual tonsil
- pharyngeal (adenoid) tonsil
- palatine or fascial tonsil
Together they form Waldeyer's ring
are lymphoid tissue
covered by respiratory epithelium
- pseudostratified ciliated
columnar epithelium
3
4. …..
produce lymphocytesproduce lymphocytes
are active in theare active in the synthesis of immunoglobulinssynthesis of immunoglobulins
a ring of lymphoid tissue in the oropharynx anda ring of lymphoid tissue in the oropharynx and
nasopharynxnasopharynx
are the first lymphoid aggregates in theare the first lymphoid aggregates in the
aerodigestive tract – thought to play a role inaerodigestive tract – thought to play a role in
immunityimmunity
4
6. Ovoid-shaped
are located laterally in the oropharynx
are bordered by the following tissues:
- Deep - Superior constrictor muscle
- Anterior - Palatoglossus muscle
- Posterior - Palatopharyngeus muscle
- Superior - Soft palate
- Inferior - Lingual tonsil
Anatomy…cont
6
7. Blood supplyBlood supply
through the externalthrough the external
carotid artery branches:carotid artery branches:
Superior poleSuperior pole
Ascending pharyngeal arteryAscending pharyngeal artery
(tonsilar branches)(tonsilar branches)
Lesser palatine arteryLesser palatine artery
Inferior poleInferior pole
Facial artery branchesFacial artery branches
Dorsal lingual arteryDorsal lingual artery
Ascending palatine arteryAscending palatine artery
7
8. …..
Venous outflowVenous outflow - by the plexus around the- by the plexus around the
tonsilar capsule, the lingual vein, and thetonsilar capsule, the lingual vein, and the
pharyngeal plexus.pharyngeal plexus.
Lymphatic drainageLymphatic drainage - the superior deep- the superior deep
cervical nodes, the jugulodigastric nodes.cervical nodes, the jugulodigastric nodes.
Sensory supplySensory supply - the glossopharyngeal nerve,- the glossopharyngeal nerve,
the lesser palatine nervethe lesser palatine nerve
8
9. Anatomic & physiologic diff btn normal Adenoid
and Tonsil
ADENOID TONSIL
1.Anatomic location posterior wall of
nasopharynx
lateral wall of oropharynx
2.Gross Triangular shape
few crypts
ovoid shape
20-30 crypts
3.microscopic Transitional antigen
processing.
No afferent fibers
Specilized antigen
processing.
No afferent fibers
4.physiology Muciliary clearance
Antigem processing
Immune survellence
Mucilliary clearance
Antigen processing
Immune survellence
9
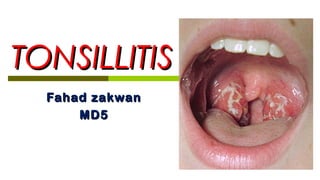
10. TonsillitisTonsillitis
Tonsillitis is inflammation of the pharyngealTonsillitis is inflammation of the pharyngeal
tonsils.tonsils.
The inflammation usually extends to theThe inflammation usually extends to the
adenoid and the lingual tonsils; therefore, theadenoid and the lingual tonsils; therefore, the
term pharyngitis may also be used.term pharyngitis may also be used.
Lingual tonsillitis refers to isolated inflammationLingual tonsillitis refers to isolated inflammation
of the lymphoid tissue at the tongue base.of the lymphoid tissue at the tongue base.
10
13. Pathophysiology and Etiology
Viral or bacterial infectionsViral or bacterial infections andand immunologic factorsimmunologic factors lead tolead to
tonsillitis and its complications. Overcrowded conditions andtonsillitis and its complications. Overcrowded conditions and
malnourishment promote tonsillitis. Most episodes of acutemalnourishment promote tonsillitis. Most episodes of acute
pharyngitis and acute tonsillitis are caused by viruses such aspharyngitis and acute tonsillitis are caused by viruses such as
the following:the following:
Herpes simplex virusHerpes simplex virus
Epstein-Barr virus (EBV)Epstein-Barr virus (EBV)
CytomegalovirusCytomegalovirus
Other herpes virusesOther herpes viruses
AdenovirusAdenovirus
Measles virusMeasles virus 13
14. Bacteria cause 15-30% of cases of pharyngotonsillitis.
Anaerobic bacteria play an important role in tonsillar
disease.
Most cases of bacterial tonsillitis are caused by group A
beta-hemolytic Streptococcus pyogenes (GABHS).
S pyogenes adheres to adhesin receptors that are located
on the tonsillar epithelium.
Immunoglobulin coating of pathogens may be important in
the initial induction of bacterial tonsillitis.
15. Mycoplasma pneumoniaeMycoplasma pneumoniae,, Corynebacterium diphtheriaeCorynebacterium diphtheriae,,
andand Chlamydia pneumoniaeChlamydia pneumoniae rarely cause acute pharyngitis.rarely cause acute pharyngitis.
Neisseria gonorrheaNeisseria gonorrhea may cause pharyngitis in sexually activemay cause pharyngitis in sexually active
persons.persons.
Arcanobacterium haemolyticumArcanobacterium haemolyticum is an important cause ofis an important cause of
pharyngitis in Scandinavia and the United Kingdom but ispharyngitis in Scandinavia and the United Kingdom but is
not recognized as such in the United States.not recognized as such in the United States.
A rash similar to that of scarlet fever accompanies AA rash similar to that of scarlet fever accompanies A
haemolyticum pharyngitis.haemolyticum pharyngitis.
15
16.
17. ACUTE TONSILITISACUTE TONSILITIS
This is the commonest URTI in children.This is the commonest URTI in children.
Occurs up to the age of 15Occurs up to the age of 15
Its common in all sexesIts common in all sexes
Viral: HSV, EBV,CMV, Adenovirus, Measles.Viral: HSV, EBV,CMV, Adenovirus, Measles.
Bacteral: anaerobes, group A beta hemolyticBacteral: anaerobes, group A beta hemolytic
strepto pyogens, mycoplasma, chlamydia,strepto pyogens, mycoplasma, chlamydia,
N.gonorrhea.N.gonorrhea.
17
18. ACUTE TONSILLITIS-TYPESACUTE TONSILLITIS-TYPES
Acute catarrhal/superficialAcute catarrhal/superficial here tonsillitis is a part ofhere tonsillitis is a part of
generalized pharyngitis, mostly seen in viral infectionsgeneralized pharyngitis, mostly seen in viral infections
Acute follicularAcute follicular infection spread into the crypts withinfection spread into the crypts with
purulent material, presenting at the opening of crypts aspurulent material, presenting at the opening of crypts as
yellow spotsyellow spots
Acute parenchymatousAcute parenchymatous tonsil in uniformly enlarged andtonsil in uniformly enlarged and
congestedcongested
Acute membranousAcute membranous follows stage of acute follicularfollows stage of acute follicular
tonsillitis where exudates coalesce to form membrane ontonsillitis where exudates coalesce to form membrane on
the surfacethe surface
22. SIGNSSIGNS
HalitosisHalitosis
Coated tongueCoated tongue
Congestion of pillars, soft palate andCongestion of pillars, soft palate and
uvulauvula
Jugulo-digastric nodes enlarged andJugulo-digastric nodes enlarged and
tendertender
Tonsils are congested and enlargedTonsils are congested and enlarged
depending on type of acute tonsillitisdepending on type of acute tonsillitis
23. TREATMENTTREATMENT
Bed restBed rest
Plenty of oral fluidsPlenty of oral fluids
AnalgesicsAnalgesics
Antimicrobial therapyAntimicrobial therapy penicillinpenicillin
In case of penicillin sensitivityIn case of penicillin sensitivity
macrolides are givenmacrolides are given
26. CHRONIC TONSILLITISCHRONIC TONSILLITIS
AetiologyAetiology::
Complication of acute tonsillitisComplication of acute tonsillitis
Sub clinical infection of tonsilSub clinical infection of tonsil
Chronic sinusitis or dental sepsisChronic sinusitis or dental sepsis
Mostly affects children and youngMostly affects children and young
adultsadults
27. TYPES OF CHRONIC TONSILLITISTYPES OF CHRONIC TONSILLITIS
Chronic follicular tonsillitisChronic follicular tonsillitis
Chronic parenchymatous tonsillitisChronic parenchymatous tonsillitis : tonsils: tonsils
are very much enlarged uniformly andare very much enlarged uniformly and
may interfere with speech, deglutition andmay interfere with speech, deglutition and
respiration, long standing cases mayrespiration, long standing cases may
develop pulmonary hypertensiondevelop pulmonary hypertension
Chronic fibroid tonsillitisChronic fibroid tonsillitis
28. CLINICAL FEATURESCLINICAL FEATURES
recurrent attacks of sore throatrecurrent attacks of sore throat
chronic irritation in throat with coughchronic irritation in throat with cough
halitosishalitosis
dysphagiadysphagia
odynophagiaodynophagia
thick speechthick speech
29. SIGNSSIGNS
Tonsil may show varying degree ofTonsil may show varying degree of
enlargement depending on the typeenlargement depending on the type
Irwin-moore signIrwin-moore sign pressure on the anteriorpressure on the anterior
pillar expresses frank pus or cheesy materialpillar expresses frank pus or cheesy material
mainly seen in fibroid typemainly seen in fibroid type
Flushing of the anterior pillar compared to restFlushing of the anterior pillar compared to rest
of the pharyngeal mucosaof the pharyngeal mucosa
Enlargement of the jugulo-digastric nodeEnlargement of the jugulo-digastric node
soft non tendersoft non tender
32. Clinical presentationClinical presentation
1.HISTORY1.HISTORY
Individuals with acute tonsillitis present withIndividuals with acute tonsillitis present with feverfever,, sore throatsore throat,,
foul breathfoul breath,, dysphagiadysphagia,, odynophagiaodynophagia andand tender cervicaltender cervical
lymph nodes.lymph nodes.
Airway obstruction may manifest asAirway obstruction may manifest as mouth breathingmouth breathing,,
snoringsnoring,, sleep-disordered breathingsleep-disordered breathing,, nocturnal breathingnocturnal breathing
pausespauses, or, or sleep apneasleep apnea..
LethargyLethargy andand malaisemalaise are common.are common.
Symptoms usually resolve in 3-4 days but may last up to 2Symptoms usually resolve in 3-4 days but may last up to 2
weeks despite adequate therapy.weeks despite adequate therapy.
32
33. Recurrent streptococcal tonsillitis is diagnosed whenRecurrent streptococcal tonsillitis is diagnosed when
an individual hasan individual has
7 culture-proven episodes in 1 year7 culture-proven episodes in 1 year,,
5 infections in 2 consecutive years5 infections in 2 consecutive years, or, or
3 infections each year for 3 years consecutively3 infections each year for 3 years consecutively..
Individuals with chronic tonsillitis may present withIndividuals with chronic tonsillitis may present with
chronic sore throatchronic sore throat,, halitosishalitosis,, tonsillitistonsillitis, and, and persistentpersistent
tender cervical nodes.tender cervical nodes.
Children are most susceptible to infection by those inChildren are most susceptible to infection by those in
the carrier state.the carrier state. 33
34. Individuals withIndividuals with peritonsillarperitonsillar
abscess (PTA)abscess (PTA) present withpresent with severesevere
throat painthroat pain,, feverfever,, droolingdrooling,, foulfoul
breathbreath,, trismustrismus (difficulty opening(difficulty opening
the mouth), andthe mouth), and altered voicealtered voice
qualityquality (the hot-potato voice).(the hot-potato voice).
34
35. 2.PHYSICAL EXAM..2.PHYSICAL EXAM..
Should begin by determining the degree of distressShould begin by determining the degree of distress
regarding airways and swallowing.regarding airways and swallowing.
Examination of pharynx may be facilitated by mouthExamination of pharynx may be facilitated by mouth
opening without tongue protrusion, followed byopening without tongue protrusion, followed by
gentle central depression of the tongue.gentle central depression of the tongue.
Full assessment of oral mucosa, dentation, andFull assessment of oral mucosa, dentation, and
salivary ducts may then be performed by gentlysalivary ducts may then be performed by gently
“walking ”a tongue depressor about the lateral oral“walking ”a tongue depressor about the lateral oral
cavity.cavity.
35
37. Flexible fiberoptic nasopharyngoscopy may be useful in
selected cases.
Acute tonsilitis reveals fever and enlarged inflammed
tonsil that may have exudates.
Open mouth breathing and voice changes result from
obstructive tonsilar enlargement.
Voice change in acute tonsilitis is not as severe as that
assc with peritonsilar abscess.
37
38. In PTA , pharyngeal edema and trismus cause a hot
potato voice.
Tender cervical nodes and neck stiffness observed in
acute tonsilitis.
Examine skine and mucosa for sign of dehydration.
Chronic tonsilitis,express pus on squeezing the tonsil and
excess tonsilar debris(tonsiliolith)
Hypertrophic inflammed tonsil for childrens and atrophic
tonsil in adult.
38
39. Tonsil in this pt were so swollen that they caused
resp distress necessitating tonsillectomy
39
43. INVESTIGATIONSINVESTIGATIONS
Tonsillitis and peritonsillar abscess (PTA) are clinical
diagnoses.
Testing is indicated when group A beta-hemolytic
Streptococcus pyogenes (GABHS) infection is suspected.
Throat cultures (sensitivity 90-95%) are the criterion
standard for detecting GABHS.
For patients in whom acute tonsillitis is suspected to have
spread to deep neck structures radiologic imaging using
plain films of the lateral neck or CT scans with contrast is
warranted.
In cases of PTA, CT scanning with contrast is indicated 43
44. Lab StudiesLab Studies
Throat cultures are the criterion standard forThroat cultures are the criterion standard for
detecting group A beta-hemolytic Streptococcusdetecting group A beta-hemolytic Streptococcus
pyogenes (GABHS).pyogenes (GABHS).
GABHS is the principal organism for which antibioticGABHS is the principal organism for which antibiotic
therapy (sensitivity 90-95%) is definitely indicated.therapy (sensitivity 90-95%) is definitely indicated.
Relying only on clinical criteria, such as the presenceRelying only on clinical criteria, such as the presence
of exudate, erythema, fever, andof exudate, erythema, fever, and
lymphadenopathy, is not an accurate method forlymphadenopathy, is not an accurate method for
distinguishing GABHS from viral tonsillitis.distinguishing GABHS from viral tonsillitis.
44
45. A rapid antigen detection test (RADT), also known asA rapid antigen detection test (RADT), also known as
the rapid streptococcal test, detects the presencethe rapid streptococcal test, detects the presence
of GABHS cell wall carbohydrate from swabbedof GABHS cell wall carbohydrate from swabbed
material and is considered less sensitive than throatmaterial and is considered less sensitive than throat
cultures;cultures;
however, the test has a specificity of 95% or morehowever, the test has a specificity of 95% or more
and produces a result in significantly less time thanand produces a result in significantly less time than
that required for throat cultures.that required for throat cultures.
A negative RADT requires that a throat culture beA negative RADT requires that a throat culture be
obtained before excluding GABHS infection.obtained before excluding GABHS infection. 45
46. ImagingImaging
Routine imaging is not useful in cases of acuteRoutine imaging is not useful in cases of acute
tonsillitis.tonsillitis.
For pts whom acute tonsillitis is suspected toFor pts whom acute tonsillitis is suspected to
have spread to deep neck structures (i.e.have spread to deep neck structures (i.e.
beyond the facial planes of thebeyond the facial planes of the
oropharynx),radiologic imaging using plainoropharynx),radiologic imaging using plain
films of lateral neck or CT scan with contrast isfilms of lateral neck or CT scan with contrast is
warranted.warranted.
46
47. Peritonsilar abscess CT scan with contrastPeritonsilar abscess CT scan with contrast
is indicated in general for unusualis indicated in general for unusual
presentation(e.g. inferior pole abscess)presentation(e.g. inferior pole abscess)
and for pts at high risk of drainageand for pts at high risk of drainage
procedures.procedures.
CTscan may be used to guide needleCTscan may be used to guide needle
aspiration for draining PTA.aspiration for draining PTA.
47
49. HistologyHistology
- If tonsils are asymmetric- If tonsils are asymmetric
- they should be submitted- they should be submitted
separatelyseparately
- examined histologically to rule- examined histologically to rule
out cancerout cancer
49
51. INDICATIONS FOR TONSILLECTOMYINDICATIONS FOR TONSILLECTOMY
The American Academy of Otolaryngology–The American Academy of Otolaryngology–
Head and Neck Surgery (AAO-HNS):Head and Neck Surgery (AAO-HNS):
Enlarged tonsils that cause upper airwayEnlarged tonsils that cause upper airway
obstruction, severe dysphagia, sleep disordersobstruction, severe dysphagia, sleep disorders
Recurrent peritonsillar abscessRecurrent peritonsillar abscess
Unilateral tonsil hypertrophy that is presumed to beUnilateral tonsil hypertrophy that is presumed to be
neoplastic (tumour tonsillectomy)neoplastic (tumour tonsillectomy)
Chronic or recurrent tonsillitis, Cor pulmonaleChronic or recurrent tonsillitis, Cor pulmonale
51
53. TONSILLECTOMYTONSILLECTOMY
Place the patient in the Rose position
with a shoulder roll.
Carefully, insert a Davis Boyle’s mouth
gauge, open and suspend it.
Apply an Alyss clamp to the tonsil to
allow for traction during dissection.
53
55. …..
Variations in dissection methods include the following
- cold steel (eg, scissors, curettes)
- monopolar cautery
- bipolar cautery
- radiofrequency ablation/coblation (can be used to shrink tonsils)
- harmonic scalpel with vibrating titanium blades
- microdebrider - for an intracapsular technique
55
56. …..
Variations in haemostasis methods include the following:
- pressure with sponge for several minutes
- bismuth subgallate
- ties
- cautery
56
58. ComplicationsComplications
HaemorrhageHaemorrhage
- the most common complication- the most common complication
- intraoperative/primary (occurring within the first 24hrs)- intraoperative/primary (occurring within the first 24hrs)
- secondary (occurring between 24hrs and 10 days)- secondary (occurring between 24hrs and 10 days)
Pain (sore throat, otalgia)Pain (sore throat, otalgia)
Dehydration (children - do not eat because of pain)Dehydration (children - do not eat because of pain)
Fever (not common, usually related to local infection)Fever (not common, usually related to local infection)
Postoperative airway obstruction (uvular oedema,Postoperative airway obstruction (uvular oedema,
haematoma, aspirated material)haematoma, aspirated material)
58
59. …..
Local trauma to oral tissuesLocal trauma to oral tissues
Temporomandibular joint dislocationTemporomandibular joint dislocation
Psychological trauma, night terrors, or depressionPsychological trauma, night terrors, or depression
Nasopharyngeal stenosisNasopharyngeal stenosis
DeathDeath
- uncommon- uncommon
- bleeding- bleeding
- or anaesthetic complications- or anaesthetic complications
59
60. Refferences….
Head & Neck ENT surgery 4th
ed
ABC of ENT
Pubmed…current articles 2013
Current diagnosis & treatment in otolaryngology..
60