Call Girls in Dwarka Mor Delhi Contact Us 9654467111
Cancer lecture
1. Cancer- today find the cause:
tomorrow find the cure
Professor E.E.U. Akang
Medical Laboratory Science Council Of Nigeria
World-wide Biomedical Laboratory Science
Day Celebration
29 April, 2009
2. What is cancer?
• A type of neoplasm (“new growth”) that
invades normal tissues and spreads
(metastasises) to distant sites, i.e.
malignant
• Clonal (arises from single abnormal cell)
• Autonomous (not subject to growth control)
• Purposeless (dysfunctional)
• Detrimental to host tissue
3. What is the global and
national burden of cancer?
• 5 million female and 6 million male new
cancer cases worldwide (of which 100,000
occur in Nigeria) annually
• >6 million deaths worldwide annually
• >50% of patients with cancer live in
developing countries, which have <10% of
the resources for cancer therapy
5. What do we know about the
history of cancer?
• Cancer is literally as old as man
• 1 Sam 5:6, GNB, “The LORD punished
the people of Ashdod…by causing them
to have tumours”
• Neolithic man 10,000 BC
• Ancient Egypt and Peru 3,000 BC
• Hippocrates 400 BC “carcinoma”
6. What do we know about
carcinogenesis?
Carcinogenesis is a multi-hit, multi-stage
process
•>80% NATURE- environment
Radiation, Chemicals, VirusesDNA/RNA, Helicobacter pylori
•<10% NURTURE- genes
Cytogenetic, Genetic, Multifactorial, Imprint
ing
7. What do we know about the
molecular genetics of cancer?
• Oncogenes
• Tumour suppressor genes
• DNA repair genes
• Metastasis genes
• Apoptosis genes
9. Breast cancer as a paradigmjustification
•
•
•
•
#1 female cancer worldwide
>1 million new cases/yr
>400,000 deaths/yr
In Nigeria, breast cancer afflicts
>12,000 women/yr
(GLOBOCAN, 2002)
10. Breast cancer is heterogeneous
Breast cancer is not a single disease, but a
spectrum of several clinical and
morphological entities, each having
distinctive natural history and prognostic
outcomes
11. Research themes in breast
cancer
•
•
•
•
Determination of cell of origin
Elucidation of molecular mechanisms
Identification of susceptibility genes
Classification of breast cancer
12. Recent advances in breast cancer
• Specific risk of malignant transformation
associated with premalignant breast
lesions
• Molecular mechanisms responsible for
invasion and metastasis
• Characteristic signatures associated with
specific subsets of breast cancer on the
basis of genetic profiling
13. Conventional tests
• Histological typing (good vs. bad
histological variants)
• Histological grading (Scarff-BloomRichardson)
• Immunohistochemical profiling
(HER2, ER and PR status)
14. Molecular tests
• Fluorescence in situ hybridisation
• Polymerase chain reaction
• Southern blotting
• Gene microarrays
These tests are applicable to surgical
biopsies, Tru-cut biopsies, FNAs, and frozen
section
16. Molecular targets in breast cancer
(Cristofanilli and Hortobagyi, 2002)
Signal
transduction
Non-hormonal
targets
Breast cancer
molecular
pathways
Cell cycle
apoptosis
Cell growth
pathways
Cell
proliferation
Angiogenesis
Hormonal
targets
Microenvironment
interaction
Nuclear
receptor family
Cell
differentiation
18. Natural and synthetic ligands of nuclear
receptor family members
RECEPTOR CATEGORY
1. STEROID
Oestrogen receptor
Progesterone
receptor
Androgen receptor
2. NON-STEROID
Vitamin D receptor
Retinoid nuclear
receptor (RAR)
Peroxisome
proliferator-activated
receptor
Farnesoid Xactivated receptor
NATURAL LIGAND
SYNTHETIC LIGANDS
Oestradiol
Progesterone
Tamoxifen
Medroxyprogesteron
e acetate, RU486
Hydroxyflutamide,
bicalutamide
Dihydroxytestosterone
1,25-dihydroxy vitamin D EB1089, CB966
Retinoic acid
All-trans-retinoic acid
15-deoxy-Δ-12,14prostaglandin J2
TGZ, LY29311
Bile acid
SR-45023A (apomine)
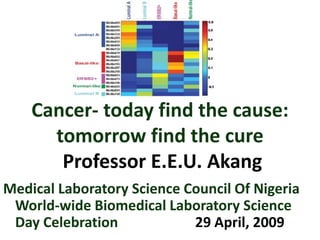
19. Molecular subtypes of breast cancer
LUMINAL B
p38 MAPK
LUMINAL A
val/leu/ile/glu
degradation
glu metabolism
VEGF
Sonic Hedgehog
Notch
G1/S checkpoint
ERBB2
Sterol biosynthesis
G1/S checkpoint
TGF-β, FGF
Toll-like receptor
T-cell receptor
IGF-1
BASAL-LIKE
NORMAL
JAK/Stat
Wnt/B-catenin
G1/S checkpoint
PDGF, EGF
Gly, ser, and thr
metabolism
PPAR
Oestrogen receptor
IFG-1
PPAR
IL-6, IL-4
NF-κB
B-cell receptor
Death receptor
20. Luminal A
• High ESR1, GATA3, HNF 3A, TFF3 , KRT8
expression (luminal cell phenotype)
• ER positive
• Relatively good prognosis (best molecular
type)
• Predicts response to methotrexate- and
paclitaxel based chemotherapy and
resistance to anthracyclines
21. Luminal B
• ER positive tumours characterised
by lower expression of luminal type
genes
• Have a relatively poor prognosis
22. Basal-like
• High expression of basal cell markers (KRT5,
KRT17, LAMC2)
• On immunohistochemical analysis, these
neoplasms are triple negative, lacking ER, PR
and HER2 expression
• Worst prognosis of all breast cancer types
• Young Hispanic and African-American
women
23. ERBB2+
• Overexpress HER2 and are oestrogen
receptor (ER) negative
• HER2 overexpression is an adverse
prognostic factor associated with
poorly-differentiated, high-grade
tumours, high proliferative rates and
lymph node involvement
• Chemoresponsive to Trastuzumab and
anthracycline-based chemotherapy
24. Normal-like
• Co-express genes of adipose tissue and
other tissues of nonepithelial origin and
genes associated more with basal epithelial
cell expression than luminal epithelial cell
expression
25. Molecular subtypes of breast cancer
LUMINAL B
p38 MAPK
LUMINAL A
val/leu/ile/glu
degradation
glu metabolism
VEGF
Sonic Hedgehog
Notch
G1/S checkpoint
ERBB2
Sterol biosynthesis
G1/S checkpoint
TGF-β, FGF
Toll-like receptor
T-cell receptor
IGF-1
BASAL-LIKE
NORMAL
JAK/Stat
Wnt/B-catenin
G1/S checkpoint
PDGF, EGF
Gly, ser, and thr
metabolism
PPAR
Oestrogen receptor
IFG-1
PPAR
IL-6, IL-4
NF-κB
B-cell receptor
Death receptor
26. Closing remarks
• A major challenge is to reconcile conventional
morphological with new molecular classification
• Molecular studies emphasise the heterogeneity
of breast cancer subtypes
• Future studies should reveal additional
information of diagnostic, therapeutic and
prognostic import
27. NIGERIA
God bless our noble fatherland,
Great land of sunshine bright,
Where brave men chose the way of peace,
To win their freedom fight.
May we preserve our purity,
Our zest for life and jollity.
God bless our noble laboratory physicians
And laboratory scientists everywhere.
Teach them to walk in unity
To build our nation dear;
Forgetting “superiority”, “strife”, or speech,
But caring always each for each.
Modified from “Things fall apart” by Chinua Achebe
This composite bar chart indicates the enormity of the problem of cancer in graphic detail. The five major cancer killers world-wide are lung cancer, female breast cancer, cancer of the large bowel, gastric cancer and male prostate cancer.
Cancer is a disease that is literally as old as man. It is conceivable that, for as long as the problem of cancer has existed, man has continually strived to determine the cause of this group of diseases and to find methods of combating the scourge of cancer. In the book of First Samuel, Chapter 5, verse 6, according to the Good News Bible, it is written “The LORD punished the people of Ashdod severely and terrified them. He punished them and the people in the surrounding territory by causing them to have tumours”. Archaeological evidence has revealed that Neolithic man living 10,000 years before Christ suffered from tumours and other diseases (Encyclopædia Brittanica, 2008). In addition, mummies from Ancient Egypt and Peru, dating from 3,000 BC show evidence of cancerous growths (Encyclopædia Brittanica, 2008). The term “carcinoma” was introduced by Hippocrates at around 400 BC to describe the gross morphological tentacle like spread of cancerous growths and the sharp pain associated with these tumours (Encyclopædia Brittanica, 2008). However, it was not until the latter half of the 18th century that scientific ideas regarding the causation of cancer emerged (Encyclopædia Brittanica, 2008).
Cancer formation is recognized to be a multistage process resulting from the cumulative effects of multiple extrinsic physical, chemical and biological agents interacting with endogenous host factors.It is estimated that cancer is contributed to in 80% of cases by largely environmental factors, and in only a minority of cases (probably less than 10%) are purely genetic factors responsible for cancer. Some environmental factors implicated in carcinogenesis include physical agents (ultraviolet, X and gamma irradiation), chemical agents (polycyclic aromatic hydrocarbons, aromatic amines/azo dyes, alkylating agents and natural carcinogens such as aflatoxins and nitrosamines), and biological agents (Hepatitis B and C viruses, Human T cell lymphoma virus type 1, Human Papilloma Virus types 16 and 18, Epstein-Barr virus and Human Herpes Virus type 8/Kaposi Sarcoma Herpes Virus, Helicobacter pylori, Schistosoma haematobium and Clonorchis sinensis, for example).The genetic contribution to cancer may be in the form of cytogenetic (structural or numerical chromosomal defects), genetic (Mendelian defects) or multifactorial (polygenic defects). Elucidation of the genetic disorders associated with many of these conditions has improved our knowledge of the pathogenesis of cancer. Apart from mutational events, epigenetic factors relating to the control of gene expression may also contribute to carcinogenesis. For instance, during chemical carcinogenesis, and in addition, in a group of inherited conditions, where a phenomenon referred to as genomic imprinting, has been noted. This operates in cases of nephroblastoma, embryonal rhabdomyosarcoma and choriocarcinoma, for example.
Five important groups of genes play a central role in oncogenesis.1. OncogenesIn normal cells, proto-oncogenes modulate cell growth and differentiation. Exposure to physical, chemical or biological carcinogens result in their activation to form cellular oncogenes which promote neoplastic proliferation.2. Tumour suppressor genesInitially dubbed anti-oncogenes, these genes are also present in normal cells, counterpoised against oncogenes, inhibiting cellular division. If these genes are partially or completely deleted or inactivated by mutation, their braking effect on cellular proliferation is released, resulting in uninhibited neoplastic growth.3. Apoptosis genesProgrammed cell death is an important mechanism of deletion of abnormal mutated cells. Mutations in bcl-2 family genes which normally inhibit (bcl-2, Bcl-XL, MCL-1) or promote (Bax, Bcl-Xs, Bak, Bad) apoptosis have also been associated with human cancer. Mutations in these genes confer a survival advantage on neoplastic cells by inhibiting apoptosis at any stage of the cell cycle.4. Metastasis genesAs a tumour progresses, its cells acquire an increasingly aggressive phenotype with invasion of surrounding tissues and subsequent metastasis. This may be related to specific mutations involving the activation of genes promoting, or the inactivation of genes inhibiting invasion and metastasis. A candidate metastasis gene is nm23, mutations of which occur in metastatic cancers, including malignant melanoma.5. DNA repair genesThe perturbations of normal daily existence, such as for example exposure of skin to ambient ultraviolet radiation, inevitably produce minor mutations in the host genome. During cell division, these mutations are detected at appropriate cell cycle checkpoints (G1/S, G2 and M) and the cell cycle is briefly interrupted, while host DNA repair mechanisms are activated. When the damage is repaired, the cell cycle resumes and mitosis can proceed. In cases where DNA repair genes are inactivated with resultant absence of specific repair enzymes, cancer is therefore prone to develop.
In the past 5 decades there have been revolutionary advances in our understanding of the origins and nature of cancer. Most of these advances are due to parallel landmark strides in our knowledge of molecular biology and genetics. For example, molecular biology has elucidated the roles of oncogenes, tumour suppressor genes, cell cycle related proteins, cell adhesion molecules and peptide regulatory factors (cytokines, chemokines and growth factors) in oncogenesis, tumour progression and metastasis, and led to introduction of novel modalities of cancer diagnosis, screening, monitoring and therapy.This diagram emphasizes in a simplistic form the multifactorial nature of cancer and immediately indicates that any strategy for tackling the problem of cancer must of necessity be multi-pronged.
There is a veritable myriad of disease entities encompassed by the rubric of cancer. It is therefore apposite to illustrate the role of basic and applied research in the shaping of treatment modalities by using just one cancer as an example. In this regard, breast cancer is the leading cause of female cancer worldwide, accounting for over 1 million new cases and over 400,000 deaths per year globally (Parkin et al, 2001; Ferlay and Parkin, 2005). In Nigeria, breast cancer afflicts an estimated 12,000 women annually (Ferlay and Parkin, 2005).
Breast cancer is not a single disease, but a spectrum of several clinically and morphologically distinct entities, with each subset of entities having distinctive natural history and prognostic outcomes (Bertucci and Birnbaum, 2008).
Therefore, several research themes must be simultaneously undertaken simultaneously in order to elucidate the aetiopathogenesis and clinicopathological aspects of breast cancer applicable to treatment and prognostication. These include determination of breast cancer cell of origin; determination of molecular alterations associated with breast cancer; identification of breast cancer susceptibility genes; and classification of breast cancer (Bertucci and Birnbaum, 2008).
Our knowledge of the molecular pathogenesis of breast cancer has expanded rapidly during the past several years (Cristofanilli and Hortobagyi, 2002). Studies have elucidated the specific risk of malignant transformation associated with premalignant breast lesions (e.g. ductal carcinoma in situ, lobular carcinoma in situ) and defined the pathophysiological molecular mechanisms responsible for invasion and metastasis. Molecular studies have also elucidated characteristic signatures associated with specific subsets of breast cancer on the basis of genetic profiling, which is expected to show better correlation with the expected response to therapy and prognosis of breast cancer than conventional histopathological characterisation.
The introduction of immunohistochemistry has remarkably expanded the scope of diagnostic histopathology. Detection of protein expression by immunohistochemistry has enabled the discovery of new markers that have diagnostic, prognostic and therapeutic value (Osin and Lakhani, 1999). There is a direct correlation between ER/PR positivity and response to hormone manipulation techniques such as oophorectomy, anti-oestrogen therapy (tamoxifen and aromatase inhibitors) (Table 1; from Geisler and Lønning, 2005). Expression of HER2 has also been demonstrated to show good correlation with response to Herceptin. In effect, in view of the predictive and prognostic utility of immunohistochemistry, it is widely recognised to be the first and most widespread application of molecular techniques in histopathology, even though not truly a molecular technique in the strict sense (Saikia et al, 2008).
Several types of molecular tests including in situ hybridisation, polymerase chain reaction, Southern blotting and gene microarrays are available and can be applied not only to routine surgical biopsies, but also to core needle biopsies and fine needle aspirates (Krishnamurthy, 2007).
A major landmark in the characterisation of breast cancer came with the introduction of molecular phenotyping of breast cancer by Perou and colleagues in Nature magazine in the year 2000.
A major landmark in the characterisation of breast cancer came with the introduction of molecular phenotyping of breast cancer by Perou and colleagues in Nature magazine in the year 2000. Generally, molecular mechanisms or pathways involved in the pathogenesis of breast cancer may be characterised as hormonal or non-hormonal (Cristofanilli and Hortobagyi, 2002). These mechanisms provide candidate targets that may be exploited in the prognostication and treatment of breast cancer.
Non-hormonal targets - Three major pathways involved in breast carcinogenesis include signal transduction, cell cycle regulation and angiogenesis (Cristofanilli and Hortobagyi, 2002). The most important signal transducers implicated in breast cancer belong to the human epidermal growth factor receptor family (HER1/erbB1, HER2/neu/erbB2, HER3/erbB3 and HER4/erbB4). HER1 and HER2 have been demonstrated to induce neoangiogenesis, which is a crucial requirement for the processes of neoplastic growth and cancer metastasis. Another important signal transduction pathway involves c-kit, which encodes for kit (CD117), a transmembrane tyrosine kinase receptor that is structurally similar to macrophage colony stimulating factor and platelet derived growth factor receptor (PDGF). Decreased c-kit expression is associated with progression of breast cancer and high PDGF levels predict for reduced survival time and response to chemotherapy in breast cancer patients (Cristofanilli and Hortobagyi, 2002). A major player in cell cycle regulation and apoptosis is P53, which has been implicated in the pathogenesis of several sporadic and familial human cancers, including breast cancer. Mutations in this tumour suppressor gene have been described in advanced, more aggressive and metastatic breast cancer and are therefore inversely correlated with survival. Finally, it is well recognised that in order for tumours to grow beyond 2mm3 in volume, they must generate a network of stromal blood vessels to provide oxygen and nutrients and eliminate carbon dioxide and waste products, a process referred to as angiogenesis or neovascularisation. It has been clearly established that higher cytosolic levels of vascular endothelial growth factor (VEGF) are associated with adverse prognosis. Other potential chemotherapeutic targets involved in angiogenesis include matrix metalloproteinases, plasminogen activators, CD44 hyaluronate receptor, laminins, integrins and type 2 cyclo-oxygenase (COX2) (Cristofanilli and Hortobagyi, 2002).
Hormonal targets - The nuclear receptor family of steroid hormone receptors includes three major groups, namely, oestrogen receptor (ER), progesterone receptor (PR), androgen receptor (AR), glucocorticoid receptor and mineralocorticoid receptor; the non-steroidal hormone receptors for thyroxine (TR), 1,25-dihydroxyvitamin D3 9VDR) and retinoids; and orphan receptors including peroxisome proliferator activated receptor (PPAR). These receptors function as ligand-inducible nuclear transcription factors. The nuclear receptor DNA binding domain consists of highly conserved 66 amino acid core domain located centrally in each nuclear receptor. The ultimate effect of receptor ligand binding is stimulation or repression of mRNA production from sensitive genes leading to changes in protein synthesis and ultimately, in cellular function (Cristofanilli and Hortobagyi, 2002). The essential roles of ER and PR in the regulation of breast cancer growth have been clearly established (Cristofanilli and Hortobagyi, 2002). Interestingly, AR expression has been linked to higher expression of specific matrix metalloproteinases (MMP-1, -7, and -11) and of tissue inhibitors of metalloproteinase 2 (TIMP-2). Patients with AR-positive breast carcinomas also have a significantly longer overall survival than those with AR-negative tumours (Gonzalez et al, 2008).
As earlier stated, breast cancer is not a single disease, but a group of several subtypes, each with a different natural history, and each requiring different treatment (Bertucci and Birnbaum, 2008; Burstein, 2005). Molecular studies have elucidated five clinically relevant subtypes of breast carcinoma (Sørlie et al, 2006). These subtypes are conserved across ethnic groups and are already evident at the ductal carcinoma in situ stage, suggesting distinct tumour progression pathways for each tumour type, as shown in Figure 3 (Polyak, 2007).
Luminal A- These are characterised by high expression of the oestrogen receptor (ESR1), as well as other genes generally co-expressed with ESR1, such as the transcription factor GATA3, hepatocyte nuclear factor 3α, the oestrogen inducible trefoil factor 3 (TFF3) and the oestrogen-induced solute carrier SLC39A6/LIV-1, many of which are typically expressed in the luminal epithelium that lines the ducts (Sørlie et al, 2006; Tongbai et al, 2008). On immunohistochemical analysis, these tumours are ER positive (Conforti et al, 2007). Patients with Luminal A tumours usually have a relatively good prognosis (Sørlie et al, 2006). ER expression is also a predictive factor for response to methotrexate- and paclitaxel based chemotherapy and for resistance to anthracyclines (Conforti et al, 2007). Overall, these neoplasms have the best prognosis (Polyak, 2007).
Luminal B- These are ER positive tumours characterised by lower expression of luminal type genes (Tongbai et al, 2008).
Basal-like- These are characterised by high expression of basal epithelial markers such as basal cytokeratin (KRT5, KRT17) and laminin (LAMC2) genes (Sørlie et al, 2006). These neoplasms tend to be associated with germline BRCA1 mutations. On immunohistochemical analysis, these neoplasms are triple negative, lacking ER, PR and HER2 expression (Conforti et al, 2007). Patients with these tumours have the worst prognosis of all breast cancer types, experiencing a relatively short disease free and overall survival period (Polyak, 2007; Sørlie et al, 2006). Triple negative breast cancer has been shown to disproportionately affect young Hispanic and African-American women (US National Institutes of Health, 2007).
ERBB2+- These are characterised both by overexpression of HER2 and by oestrogen receptor (ER) negativity (Conforti et al, 2007). Population-based studies and retrospective analyses have shown that overexpression of HER2 is an adverse prognostic factor that is associated with poorly differentiated high-grade tumours, high proliferative rates, lymph node involvement and chemoresponsiveness to Trastuzumab and anthracycline based chemotherapy (Burstein, 2005).
Normal-like- These are characterised by expression of a large number of genes normally expressed in adipose tissue and other tissues of nonepithelial origin and higher expression of genes associated more with basal epithelial cell expression than luminal epithelial cell expression (Tongbai et al, 2008).
This figure recapitulates the five major molecular types of breast cancer and the classes of genes demonstrated in them with molecular profiling.
A major challenge is how to reconcile conventional morphological classification with the new molecular one, since there are no standardised immunohistochemical markers for assigning molecular class to a new case. One approach simply assigns new names to previous recognised subsets of breast cancers. Thus, ER-positive tumours became luminal cancers, and ER-negative, progesterone receptor-negative and HER2-negative (triple negative) tumours are considered to be basal-like carcinomas. However, this approach has several limitations. For example, there is great heterogeneity in ER-positive tumours, regarding ER-expression levels, morphological characteristics and associated molecular alterations. Thus, tumours with very distinct morphological and molecular features, such as invasive lobular carcinomas (classic type) and some grade 3 invasive ductal carcinoma will be included in the same group. The ``triple negative'' approach ignores the expression of basal markers, such as basal cytokeratins in the definition of basal-like carcinomas. In addition, several morphological studies have demonstrated that very different breast carcinomas such as some grade 3 invasive ductal carcinomas, medullary carcinomas and metaplastic carcinomas, including carcinosarcomas, expressed basal markers. Regarding the cellular origin of breast cancer, it has been recently suggested that the transformation of different subsets of stem and progenitor cells results in the diversity of breast cancer phenotypes, including the expression of basal and luminal markers and oestrogen receptors in breast cancer subtypes. Whether different types of breast carcinomas derived either from luminal or myoepithelial cell, or are the result of luminal cell plasticity or stem/progenitor cell transformation is the subject of great debate and research (Palacios, 2007).