Left ventricular failure with parkinsons disease and hypertension with type 2 dm
•Als PPTX, PDF herunterladen•
3 gefällt mir•1,648 views

A good Case presentation on pharmaceutical care plan of LVF with PD for clinical pharmacists

Empfohlen
Empfohlen
Weitere ähnliche Inhalte
Was ist angesagt?
Was ist angesagt? (10)
Andere mochten auch
Andere mochten auch (10)
Ähnlich wie Left ventricular failure with parkinsons disease and hypertension with type 2 dm
Ähnlich wie Left ventricular failure with parkinsons disease and hypertension with type 2 dm (20)
Mehr von Dr. Abhimanyu Prashar
Mehr von Dr. Abhimanyu Prashar (20)
Kürzlich hochgeladen
Kürzlich hochgeladen (20)
Left ventricular failure with parkinsons disease and hypertension with type 2 dm
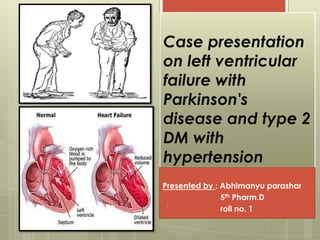
- 1. Case presentation on left ventricular failure with Parkinson's disease and type 2 DM with hypertension Presented by : Abhimanyu parashar 5th Pharm.D roll no. 11
- 2. IP no. : 223050 UNIT : medicine 1 AGE : 70 yrs SEX : Female Thursday, September 05, 2013 2
- 3. Reasons for admission : c/o : Generalized weakness x 2 days Inability to move x 2 days Thursday, September 05, 2013 3
- 4. General examination An elderly female , moderately built and nourished , conscious and cooperative Pulse : 94 BPM BP :140/90 mmHg SPo2 : 94% CBG : 169 mg/dl No meningeal signs Thursday, September 05, 2013 4
- 5. Pallor + No cyanosis , no clubbing CNS : cranial nerves normal P/A : soft and non tender Power : Tone : Thursday, September 05, 2013 5 U/L L/L R 3/5 3/5 L 4/5 4/5 U/L L/L R N N L N N
- 6. DTR : Thursday, September 05, 2013 6 RIGHT LEFT B +++ ++ T ++ ++ S ++ ++ K +++ ++ A +++ ++ Plantar increased Normal
- 8. PMHx : K/C/O type 2 DM x 8 years and was on glimipride and metformin (½-0-0) K/C/O hypertension x 8 yrs and was on losartan (1-0-0) H/O of seizures disorders . Thursday, September 05, 2013 8
- 9. Thursday, September 05, 2013 9 Allergies FHx SHx NKA NS NS
- 10. Personal history DIET : veg APPETITE : good SLEEP : undisturbed BOWEL and BLADDER : normal and regular Thursday, September 05, 2013 10
- 11. PROVISIONAL DIAGNOSIS TYPE 2 DM with TRANSIENT ISCHEMIC ATTACK Thursday, September 05, 2013 11
- 12. DAY NOTES : Thursday, September 05, 2013 12
- 13. DAY 1 BP : 140/80 mmHg PULSE : 94 BPM SPo2 : 94% CBG :169 mg/dl C/O : generalized weakness since 2 days Unable to move around since 2 days Difficulty in moving all 4 limbs Thursday, September 05, 2013 13
- 14. O/E : CVS: S1S2 present and no murmurs RS: NVBS + , no added sounds CNS: Patient is conscious oriented and cranial nerves are normal No atrophy or hypertrophy of muscles ADV : treatment as per chart , Hb ,TC , DC , RBS , Urea , electrolytes Thursday, September 05, 2013 14
- 15. LAB REPORTS : Thursday, September 05, 2013 15
- 16. Thursday, September 05, 2013 16 Hematology Hb 9.7 g% RBC 4.18 million cells/cumm PLT 1.17 L/cumm WBC 4300 DLC : N 65% E 04% B 31% L 00% M 00% Electrolytes Na 144 mmol/l (135-147) K 4.8 mmol/l (3.5-5.0) Cl 102 mmol/l (95-105) HbA1C 10.6 (4.0-6.0) RBS 73 mg/dl (70-150) Urea 20 mg/dl (0-40) Urine analysis Pus cells 2-4 Epithelial cells 1-2 IMP : microcytic hypo chromic anemia with thrombocytopenia
- 17. TREATMENT Thursday, September 05, 2013 17 DRUGS DOSE ROUTE FREEQUENCY Inj. Actrapid 6-6-6 units SC 1-1-1 Tab. atorvastatin 40 mg PO 0-0-1 Tab. Aspirin and clopidogrel 150 mg PO 0-1-0
- 18. DAY 2 BP : 140/90 mm Hg PULSE : 92 BPM CBG : 107 mmHg O/E : CVS / RS – NAD PA : soft and non tender ADV : treatment as per chart , LFT , CKMB , Troponin-I , ortho-opinion for knee osteoarthritis. Ortho ADV : X ray for both knee standing Thursday, September 05, 2013 18
- 19. Thursday, September 05, 2013 19 LFT AST 94 (0-40) ALT 41 (0-40) ALP 665 (37-147) Billirubin Total 2.60 mg/dl(0.1-1.0) Direct 1.30 mg/dl(0-0.2) Biochemistry RBS 216 mg/dl FBS 93 mg/dl PLT 98000 cells/cumm Lipid profile HDL 35 mg/dl (30-70) LDL 43 mg/dl (60-130) VLDL 16 mg/dl (5-40) TG 82 mg/dl (10-190) Cardiac enzymes CKMB 44 U/L (0-20) Troponin I 0.002 ng/ml (Less than 0.035 ng/ml)
- 20. IgM dengue : NS 1 Ag : negative IgM anti dengue : not detected Widal test : negative QBC-MP : negative Thursday, September 05, 2013 20
- 21. TREATMENT DRUGS DOSE ROUTE FREEQUENCY Inj. Actrapid 6-6-6 units SC 1-1-1 Tab. Atorvastatin 40 mg PO 0-0-1 Tab. aspirin and clopidogrel 150 mg PO 0-1-0 Inj.trineurosol .H 1 cc IV 1-0-0 Thursday, September 05, 2013 21
- 22. DAY 3 BP : 140/90 mm Hg PULSE : 82 BPM O/E : CVS/RS – NAD ADV : 2-D ECHO , Carotid doppler, Optho opinion Thursday, September 05, 2013 22
- 23. Ophthalmology opinion : IMP : no evidence of diabetic nephropathy Thursday, September 05, 2013 23 Normal fundus
- 24. TREATMENT DRUGS DOSE ROUTE FREEQUENCY Inj. Actrapid 6-6-6 units SC 1-1-1 Tab. atorvastatin 40 mg PO 0-0-1 Tab. aspirin and clopidogrel 150 mg PO 0-1-0 Inj. Trineurosol.H 1 cc IV 1-0-0 Thursday, September 05, 2013 24
- 25. DAY 4 BP : 140/80 mm Hg PULSE : 82 BPM RS/CVS : NAD Thursday, September 05, 2013 25
- 26. At 6:15 PM Not conscious , not responding to oral commands from afternoon BP : 140/70 mmHg Pulse : 72 BPM SpO2 : 97% CVS : S1S2 + no murmurs RS : NVBS + CNS : responds to deep painful stimuli Thursday, September 05, 2013 26
- 27. Motor system : B/L plantar extension Reflex : ADV : CT scan , ECG , shift to emergency ward , ABG , U/C , SE Thursday, September 05, 2013 27 Right Left Upper limb Decreased Present Lower limb Absent Decreased
- 28. Thursday, September 05, 2013 28 Prothrombin time Control 13.5 sec Patient 30.2 sec Ratio 2.22 Index 44.7 INR 2.223 (0.8-1.2) electrolytes Na 138 mmol/l K 3.6 mmol/l Cl 104 mmol/l Ca 9.0 mmol/l (8.8-10.8) P 3.6 mmol/l (2.5-5.0) Mg 1.7 mmol/l (1.7-2.7) LFT AST 170 ALT 104 ALP 560 Billirubin – total 1.60 direct 1.14 biochemistry Urea 36 mg/dl S. Cr 1.0 mg/dl (0.8-1.4) Total protein 7.0 g/dl(6-8) Albumin 4.0 g/dl (3.4-5.0) A/G 1.3 (1.2-2.5) GFR :49.6 ml/min
- 29. ABG report pH 7.48 (7.34-7.44) PCo2 24.4 (35-45 mmHg) HCo3 18.1(22–26 mEq/L) PO2 107.5 (75-100 mmHg) BE -4.3 (−2 to +2 mmol/L) TCo2 18.9(100-132mg/dl) Thursday, September 05, 2013 29
- 30. TREATMENT Thursday, September 05, 2013 30 DRUGS DOSE ROUTE FREEQUENCY Inj. Actrapid 6-6-6 units SC 1-1-1 Tab. atorvastatin 40 mg PO 0-0-1 Tab. aspirin and clopidogrel 150 mg PO 0-1-0 Inj. Trineurosol.H 1 cc IV 1-0-0 Tab. piracetam 400 mg PO Q8H R.T. feeds 200 ml Q3H
- 31. DAY 5 BP : 140/80 mm Hg PULSE : 108 BPM SpO2 : 98% CBG : 130 mg/dl O/E : Patient responds to simple oral commands , eye movements + Afebrile , no pedal edema Thursday, September 05, 2013 31
- 32. CVS : S1S2 + , no murmur R/S : B/L NVBS + , no added sounds CNS : patient responds to verbal commands B/L plantar withdrawal Pupil : reactive Moves all 4 limbs . Mild terminal neck stiffness. Doll eye movement + Cough reflex + Thursday, September 05, 2013 32
- 33. ECG : heart rate 100 / minute Sinus rhythm + axis . T inversion V2V6 ADV : RT feeding 200 ml Q3H , perform CBG Q8H , IVF NS@ 30 ml/Hr , weil Felix test Weil felix test : negative CST and neurologist opinion . NEURO OPINION : Pt stuporous , max response to painful stimuli , maximum movements of limbs Add SYNDOPA (LEVODOPA + carbidopa) 110 mg ½ ½ ½ CT head : not significant ADV : LP-CSF analysis , may require MRI scan Thursday, September 05, 2013 33
- 35. TREATMENT Thursday, September 05, 2013 35 DRUGS DOSE ROUTE FREEQUENCY Inj. Actrapid 6-6-6 units SC 1-1-1 Tab. atorvastatin 40 mg PO 0-0-1 Tab. aspirin and clopidogrel 150 mg PO 0-1-0 Inj. Trineurosol.H 1 cc IV 1-0-0 Tab. piracetam 400 mg PO Q8H R.T. feeds 200 ml Q3H T.syndopa 110 mg PO ½ ½ ½
- 36. DAY 6 BP : 140/80 mm Hg PULSE : 100 BPM O/E : patient responds to oral commands by opening eye SPO2 : 98% CVS : S1S2 + , no murmurs RS : B/L NVBS + CNS : patient stuporous , response to painful stimuli , B/L plantar -- Thursday, September 05, 2013 36
- 37. B/L : pupil 4 mm reactive , doll eye movement + , cough reflex + ADV : Repeat PLT count , USG abdomen , CXR- PA view , MRI brain USG abdomen : normal MRI report : old infarction , doesn't explain clinical state Thursday, September 05, 2013 37
- 38. Thursday, September 05, 2013 38 CXR - PA view showing NORMAL and CARDIAC HYPERTROPHY
- 39. TREATMENT Thursday, September 05, 2013 39 DRUGS DOSE ROUTE FREEQUENCY Inj. Actrapid 6-6-6 units SC 1-1-1 Tab. Atorvastatin 40 mg PO 0-0-1 Tab. aspirin and clopidogrel 150 mg PO 0-1-0 Inj. Trineurosol.H 1 cc IV 1-0-0 Tab. Piracetam 400 mg PO Q8H tab. Doxycyclin 100 mg PO ½- ½ - ½ R.T. feeds 200 ml Q3H T.syndopa 110 mg PO ½ ½ ½
- 40. DAY 7 BP : 160/80 mm Hg PULSE : 102 BPM SPO2 : 98% O/E : patient responds to oral commands with comprehensive sounds Spontaneous movements of all 4 limbs CVS : S1S2 + no murmurs Thursday, September 05, 2013 40
- 41. RS : B/L NVBS + no added sounds PA: soft and no organomegaly ECG : ST and T wave changes CNS : patient responds to deep pain stimulation , spontaneous of all 4 limbs + B/L plantar withdrawal , Cog-wheal rigidity : + GCS : 8/15 Thursday, September 05, 2013 41
- 42. Thursday, September 05, 2013 42 1 2 3 4 5 6 Eyes Does not open eyes Opens eyes in response to painful stimuli Opens eyes in response to voice Opens eyes spontane ously N/A N/A Verbal Makes no sounds Incompr ehensible sounds Utters inapprop riate words Confuse d, disorient ed Oriented, converses normally N/A Motor Makes no moveme nts Extensio n to painful stimuli Abnorm al flexion to painful stimuli Flexion / Withdra wal to painful stimuli Localizes painful stimuli Obeys comman ds Glasgow Coma Scale . The lowest possible GCS (the sum) is 3 (deep coma or death), while the highest is 15 (fully awake person). brain injury is classified as: •Severe, with GCS < 9 •Moderate, GCS 9–12 •Minor, GCS ≥ 13.
- 43. B/L : pupil 4 mm and reactive ADV : repeat platelet count, U/C , S/E , LP, CSF analysis . At 3:00 PM call attended for LP LP is done in L3 and L4 interspace Thursday, September 05, 2013 43 Clear and free flow of CSF , 24 drops each in 3 containers Post procedure : BP – 140/90 mmHg PULSE – 100 BPM SPO2 : 99% RS – B/L NVBS +
- 44. RBS 45 mg/dl (40-70) Protein 20 mg/dl (20-45) Chlorine 112 mg/dl (116-122 mg/dl) Thursday, September 05, 2013 44 CSF analysis report 0.1 ml clear fluid Cell count : 3 cells/cumm Cell type : a few lymphocytes Non malignant cells in smear CSF analysis report Gram stain No cells no organism ZN stain No AFB India ink No cryptococcus
- 45. PLT 1.09 Lakhs/cumm UREA 22 mg/dl S.Cr 0.8 mg/dl Thursday, September 05, 2013 45 electrolytes Na 128 mmols/L K 3.6 mmols/L Cl 103 mmols/L
- 46. TREATMENT Thursday, September 05, 2013 46 DRUGS DOSE ROUTE FREEQUENCY Inj. Actrapid 6-6-6 units SC 1-1-1 Tab. atorvastatin 40 mg PO 0-0-1 Tab. aspirin and clopidogrel 150 mg PO 0-1-0 Inj. Trineurosol.H 1 cc IV 1-0-0 Tab. piracetam 400 mg PO Q8H tab. Doxycyclin 100 mg PO ½- ½ - ½ R.T. feeds 200 ml Q3H T.syndopa 110 mg PO ½ ½ ½
- 47. DAY 8 BP : 170/100 mm Hg PULSE : 98 BPM O/E : CVS : S1S2+ , no murmurs Input/output : 2000/4000 FCBG : 130 mg/dl Pre dinner : 138 mg/dl RS : B/L NVBS + Thursday, September 05, 2013 47
- 48. CNS : responds to deep pain stimuli B/L plantar – Cog-wheel rigidity : + B/L pupil : 4 mm and reactive ECG : T wave inversion in V2 and V4 (ischemic) ST flat in II and III , avf ,V3 and V6 Thursday, September 05, 2013 48
- 49. TREATMENT Thursday, September 05, 2013 49 DRUGS DOSE ROUTE FREEQUENCY Inj. Actrapid 6-6-6 units SC 1-1-1 Tab. atorvastatin 40 mg PO 0-0-1 Tab. aspirin and clopidogrel 150 mg PO 0-1-0 Inj. Trineurosol.H 1 cc IV 1-0-0 Tab. piracetam 400 mg PO Q8H tab. Doxycyclin 100 mg PO ½- ½ - ½ R.T. feeds 200 ml Q3H T.syndopa 110 mg PO ½ ½ ½
- 50. DAY 9 BP : 140/70 mmHg PULSE : 84 BPM SPO2 : 94% ECG : t wave inversion an V1 and V6 CVS : S1S2 + , no murmurs RS : B/L NVBS + , no added sounds CNS : conscious oriented , responds to commands Thursday, September 05, 2013 50
- 51. POWER : 4/5 Cog-wheel rigidity : + GCS : 9/15 B/L pupil : 4 mm and reactive B/L plantar : flexion ADV : 2D-ECHO Thursday, September 05, 2013 51
- 52. ECHO report Mildly dilated cardiac chambers Mild apical-septal hypokinesia Decreased LV systolic dysfunction EF : 36% LV diastolic dysfunction Sclerotic aortic valves with no significant stenosis ( age related) Thursday, September 05, 2013 52
- 54. TREATMENT Thursday, September 05, 2013 54 DRUGS DOSE ROUTE FREEQUENCY Inj. Actrapid 6-6-6 units SC 1-1-1 Tab. atorvastatin 40 mg PO 0-0-1 Tab. aspirin and clopidogrel 150 mg PO 0-1-0 Inj. Trineurosol.H 1 cc IV 1-0-0 Tab. piracetam 400 mg PO Q8H tab. Doxycyclin 100 mg PO ½- ½ - ½ T.syndopa 110 mg PO ½ ½ ½
- 55. DAY 10 BP: 120/80 , 140/70 mmHg PULSE : 90 BPM FCBG : 91 mg/dl Pre lunch : 169 mg/dl Pre dinner : 140 mg/dl O/E : patient is feeling better , conscious , responds well to commands can be shifted to ward Thursday, September 05, 2013 55
- 56. RS : B/L NVBS + CNS : conscious oriented Power : 4/5 , all 4 limbs B/L plantar – B/L pupil Normal and non reactive ECG : HR – 100/ mt ST INVERSION with T wave inversion an V2 an V6 ADV : shift to ward and CST Thursday, September 05, 2013 56
- 57. TREATMENT Thursday, September 05, 2013 57 DRUGS DOSE ROUTE FREEQUENCY Inj. Actrapid 6-6-6 units SC 1-1-1 Tab. Atorvastatin 40 mg PO 0-0-1 Tab. aspirin and clopidogrel 150 mg PO 0-1-0 Inj. Trineurosol.H 1 cc IV 1-0-0 Tab. Piracetam 400 mg PO Q8H Tab . Doxycyclin 100 mg PO ½- ½ - ½ Ranolazine 500 mg PO 1-0-1 T.syndopa 110 mg PO ½ ½ ½
- 58. DAY 11 BP : 130/70 mmHg PULSE : 88 BPM O/E CVS / RS – NAD CNS : conscious oriented , POWER : 4/5 FCBG : 102 mg/dl Pre dinner : 189 mg/dl Bed sore : + ADV : wound care and CST Thursday, September 05, 2013 58
- 59. TREATMENT Thursday, September 05, 2013 59 DRUGS DOSE ROUTE FREEQUENCY Inj. Actrapid 6-6-6 units SC 1-1-1 Tab. atorvastatin 40 mg PO 0-0-1 Tab. aspirin and clopidogrel 150 mg PO 0-1-0 Tab. piracetam 400 mg PO Q8H Tab. Ramipril 2.5 mg PO 1-0-0 Cap. Cobadex PO 0-1-0 ranolazine 500 mg PO 1-0-1 T.syndopa 110 mg PO ½ ½ ½
- 60. DAY 12 BP : 120/80 mmHg PULSE : 84 BPM CVS/RS : NAD PA : soft CNS : conscious oriented ADV : neurology opinion , CST , remove IV line Thursday, September 05, 2013 60
- 61. TREATMENT Thursday, September 05, 2013 61 DRUGS DOSE ROUTE FREEQUENCY Inj. Actrapid 6-6-6 units SC 1-1-1 Tab. atorvastatin 40 mg PO 0-0-1 Tab. aspirin and clopidogrel 150 mg PO 0-1-0 Tab. piracetam 400 mg PO Q8H Tab. Ramipril 2.5 mg PO 1-0-0 Cap. Cobadex PO 0-1-0 ranolazine 500 mg PO 1-0-1 T.syndopa 110 mg PO ½ ½ ½
- 62. DAY 13 BP : 120/70 mmHg PULSE : 88 BPM O/E : patient conscious oriented Bed sore + CVS : S1S2 heard RS : NVBS + FCBG : 103 mg/dl Pre dinner : 91 mg/dl ADV : CST Thursday, September 05, 2013 62
- 63. DAY 14 BP : 130/70 mmHg PULSE : 80 BPM Seen by neurologist O/E : responds to commands , rigidity of limbs + , no tremors , mask like face + Imp : early parkinsonism ADV : tab rasagiline 0.5 mg 0-1-0 Tab. Pramipexole 0.25 mg 1-0-1 Physiotherapy and CST Patient discharged against medical advice Thursday, September 05, 2013 63
- 64. Thursday, September 05, 2013 64 Drugs D R F 1 2 3 4 5 6 7 8 9 1 0 1 1 1 2 1 3 1 4 Inj. Actrapid 6-6-6 units SC 1-1-1 + + + + + + + + + + + T. Atorvastatin 40 mg PO 0-0-1 + + + + + + + + + + + + + + T. aspirin and clopidogrel 150 mg PO 0-1-0 + + + + + + + + + + + + + + Inj. Trineurosol.H 1 cc IV 1-0-0 + + + + + + + + + T. Piracetam 400 mg PO Q8H + + + + + + + + + + + T. syndopa 110 mg PO ½ ½ ½ + + + + + + + + + + R.T. feeds 200 ml Q3H + + + + + + + + + + + + Treatment chart
- 65. Thursday, September 05, 2013 65 Drugs D R F 1 2 3 4 5 6 7 8 9 1 0 1 1 1 2 1 3 1 4 Tab. doxycycllin 100 mg Po ½ -½ - ½ + + + + + T. Ramipril 2.5 mg Po 1-0-0 + + + + + Cap. Ranolazine 500 mg Po 1-0-1 + + + + + Cap. Cobadex forte Po 0-1-0 + + + + H. mixtard 12-0-16 units SC + + T. rasagiline 0.5 mg Po 0-1-0 + Tab. pramipraxol e 0.25 mg po 1-0-1 +
- 66. PHARMACEUTICAL CARE PLAN (SOAP) Thursday, September 05, 2013 66
- 67. SUBJECTIVE EVIDENCE Thursday, September 05, 2013 67 Diabetes Parkinson's disease •Generalized weakness •Inability to move around •Reduced power •Stupor present •Mask like face
- 68. OBJECTIVE EVIDENCE Thursday, September 05, 2013 68 Hypertension Diabetes Parkinson's disease •Elevated blood pressure •Elevated blood glucose levels •Cog wheal rigidity Heart failure •2-D ECHO report ( EF 36% ) •Elevated AST •Elevated CKMB •ECG changes ( ST segment and T wave inversion)
- 69. FINAL DIAGNOSIS Based on objective and subjective evidence the patient was diagnosed as early Parkinson's disease with left ventricular failure and type 2 Diabetes mellitus and hypertension Thursday, September 05, 2013 69
- 70. GOALS OF TREATMENT Thursday, September 05, 2013 70
- 71. For DIABETES to keep patients free of symptoms associated with hyperglycemia or hypoglycemia (hunger, anxiety, palpitations, sweatiness). primary goals of DM management are to reduce the risk for microvascular and macrovascular complications to reduce mortality, and to improve quality of life Thursday, September 05, 2013 71
- 72. Thursday, September 05, 2013 72 Index Goal HB.A1C <7.0 Preprandial capillary plasma glucose 5.0–7.2 mmol/L (90–130 mg/dL) Peak postprandial capillary plasma glucose <10.0 mmol/L (<180 mg/dL) Blood pressure <130/80 Low-density lipoprotein <2.6 mmol/L (<100 mg/dL) High-density lipoprotein >1.1 mmol/L (>40 mg/dL) Triglycerides <1.7 mmol/L (<150 mg/dL) Treatment Goals for Adults with Diabetes
- 73. For HYPERTENSION Treat systolic blood pressure to recommended goal as primary focus (especially in patients older than 50 years). Individualize all therapies based on compelling indications and comorbid conditions. Ultimate treatment goal is the reduction of cardiovascular and renal morbidity and mortality Thursday, September 05, 2013 73
- 74. For CHF Minimize or prevent acute CHF exacerbations Slow progression of CHF Increase survival Thursday, September 05, 2013 74
- 75. For PARKINSONS DISEASE Improve motor function Maintain ability to complete daily activities independently Improve non-motor symptoms Maintain quality of life Thursday, September 05, 2013 75
- 76. Thursday, September 05, 2013 76 TREATMENT OPTIONS For cardiac complications For diabetes For Parkinson's disease ACE inhibitors •Ramipril Anti anginals •Ranolazine Anti hyper lipidemic •Atorvastatin Anti platelets •aspirin and clopidogrel Insulin •Human actrapid •Human mixtard Dopamine analogue •Levdopa MAO inhibitors •rasagiline Adjuvent treatments •Piracetam •Vitamin supplements
- 77. GOALS ACHIEVED Signs and symptoms were improved BP was controlled and brought WNL Blood glucose was controlled and brought WNL Patient gained consciousness Thursday, September 05, 2013 77
- 78. PROBLEMS IDENTIFIED Use of aspirin + clopidogrel in patient with thrombocytopenia Use of doxycyclin even when weil felix test was –ve PT/INR and cardiac enzymes were not repeated Thursday, September 05, 2013 78
- 79. MONITORING PARAMETERS Thursday, September 05, 2013 79 Disease related 1. Blood pressure 2. Blood glucose 3. HbA1C 4. ECG 5. Cardiac enzymes 6. Electrolytes 7. Motor symptoms
- 80. Thursday, September 05, 2013 80 Drug related For insulin : Monitor hypoglycemic symptoms Monitor for lipid-dystrophy • For ramipril : Monitor serum potassium levels Monitor blood pressure • For Levodopa : Monitor for motor symptoms and rigidity • For Aspirin and clopidogrel : Monitor blood platelet count • For Atorvastatin : Monitor plasma lipid levels
- 81. PATIENT COUNSELLING Thursday, September 05, 2013 81
- 82. About the disease(hypertension) Thursday, September 05, 2013 82
- 83. Thursday, September 05, 2013 83 About the disease(Diabetes) Signs and symptoms complications
- 84. Thursday, September 05, 2013 84 About the disease(heart failure)
- 85. Thursday, September 05, 2013 85 About the disease (PD)
- 86. About medication Name and purpose Dose and frequency Medication adherence Possible adverse effects Missed dose Thursday, September 05, 2013 86
- 88. About life style modification Thursday, September 05, 2013 88 Healthy life style with daily exercise (the ADA recommends 150 min/week (distributed over at least 3 days) of aerobic physical activity) Self-Monitoring of Blood Glucose Nutritional recommendations
- 89. Thursday, September 05, 2013 89 DASH diet
- 90. Thursday, September 05, 2013 90 Fat 20–35% of total caloric intake Saturated fat < 7% of total calories <200 mg/day of dietary cholesterol Two or more servings of fish/week provide -3 polyunsaturated fatty acids Carbohydrate 45–65% of total caloric intake (low-carbohydrate diets are not recommended) Sucrose-containing foods may be consumed with adjustments in insulin dose Protein 10–35% of total caloric intake (high-protein diets are not recommended) Other components Fiber-containing foods may reduce postprandial glucose excursions Nonnutrient sweeteners
Hinweis der Redaktion
- Generally, brain injury is classified as:Severe, with GCS < 9Moderate, GCS 9–12 (controversial)Minor, GCS ≥ 13.