Acid peptic disease (VK)
•Als PPT, PDF herunterladen•
20 gefällt mir•8,325 views


Empfohlen
Weitere ähnliche Inhalte
Was ist angesagt?
Was ist angesagt? (20)
Andere mochten auch
Andere mochten auch (20)
Ähnlich wie Acid peptic disease (VK)
Ähnlich wie Acid peptic disease (VK) (20)
Mehr von Dr. Abhavathi Vijay Kumar
Mehr von Dr. Abhavathi Vijay Kumar (20)
Kürzlich hochgeladen
Kürzlich hochgeladen (20)
Acid peptic disease (VK)
- 1. Drugs used for acid peptic disease
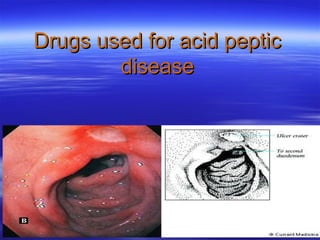
- 2. Introduction Acid peptic disorders include a number of conditions whose pathophysiology is believed to be the result of damage from acid and peptic activity in gastric secretions. It include gastroesophageal reflux, peptic ulcer (gastric and duodenal), and stress-related mucosal injury. In all these conditions, mucosal erosions or ulceration arise when the caustic effects of aggressive factors overwhelm the defensive factors of the gastrointestinal mucosa
- 3. Pathogenesis Therapy is directed at enhancing host defense or eliminating aggressive factors; i.e., H. pylori. Aggressive Factors Defensive Factors Acid, pepsin Mucus, bicarbonate layer Bile salts Blood flow, cell renewal Drugs (NSAIDs) Prostaglandins H. pylori Phospholipid
- 5. Gastric Acid Secretion Acid secretion can be viewed as under basal and stimulated conditions Basal acid production occurs in a circardian pattern with highest levels occurring during night Cholinergic and histaminergic inputs are main contributors to basal acid secretion Gastrin (after the meals) is the main stimulant for increased acid secretion
- 6. Gastric Acid Secretion (Basal) Resting Proton pumps are located within canaliculus and in Canaliculus cytoplasmic tubulovesicles H+, K+-ATPase The distribution of proton pumps between canaliculus and vesicles varies according to cell activity Under resting conditions Tubulovesicles only 5% pumps are within canaliculus
- 7. Gastric Acid Secretion (Stimulated) Stimulated Canaliculus HCl H+, K+-ATPase KCl H3O+ Gastrin Ca KCl AMP c ACh Histamine Active Pumps On stimulation of parietal cell (after a meal) 60-70% pumps are transferred to canaliculus membrane. Once cell activation stops, pumps are recycled back to cytoplasmic vesicles The tubulovesicular pumps are inactive
- 8. Regulation of gastric acid secretion at the cellular level
- 10. Drugs Therapy 1.Drugs which reduce gastric acid secretion H2-Receptors antagonists Proton pump inhibitors Anticholinergics Prostaglandin agonists
- 11. Drugs Therapy 2.Mucosal protective agents 3.Drugs which neutralise gastric acid(Antacids) 4. Ulcer healing drugs 5.Antibiotics for H. pylori eradication
- 12. H2-Receptor Antagonists Exhibit competitive inhibition at the parietal cell H2 receptor, and suppress basal and mealstimulated acid secretion in a linear, dosedependent manner. The volume of gastric secretion and concentration of pepsinare also reduced. Reduce acid secretion stimulated by histamine as well as by gastrin and cholinomimetic agents.
- 13. H2-Receptors Antagonists Inhibit 60–70% of total 24-hour acid secretion in usual prescription doses. They block more than 90% of nocturnal acid but only 60–80% of daytime acid secretion. Nocturnal and fasting intragastric pH is raised to 4–5 but the impact upon the daytime, mealstimulated pH profile is less.
- 14. Clinical Comparisons of H2 Receptor Blockers. Drug Relative Potency Dose to Achieve >50% Acid Inhibition for 10 hrs Dose for Acute Duodenal or Gastric Ulcer Dose for Dose for Gastro Prevention of eosophage Stress-Related al Reflux Bleeding Disease Cimetidine 1 400–800 mg 800 mg HS or 400mg bid 800 mg bid 50 mg/h Continuous inf Ranitidine 4-10 150 mg 300 mg HS or 150 mg bid 150 mg bid 6.25 mg/h Continuous inf or 50mg IV every 6– 8h Nizatidine 4-10 150mg 300 mg HS or 150mgbid 150 mg bid Not available Famotidine 20-50 20mg 40 mg HS or 20 mg bid 20 mg bid 20 mg IV every 12hr
- 15. H2-Receptors Antagonists Pharmacokinetics Rapidly absorbed 1-3 hrs to peak Ranitidine & Cimetidine hepatically metabolized whereas Famotidine & Nizatidine are renally excreted Dose adjustment is needed in some renal & hepatic failure patients
- 16. H2-Receptors Antagonists Side Effects Usually minor; include headache, dizziness, diarrhea, & muscular pain Hallucinations & confusion in elderly patients; Cimetidine elevates serum prolactin & alters estrogen metabolism in men Gynecomastia or impotence in men and Galactorrhea in women.
- 17. H2-Receptors Antagonists Although there are no known harmful effects on the fetus, these agents cross the placenta. Therefore, they should not be administered to pregnant women unless absolutely necessary. Secreted into breast milk and may therefore affect nursing infants .
- 18. PROTON PUMP INHIBITORS Most potent suppressors of gastric acid secretion which act by inhibiting gastric H+,K+ATPase (proton pump) In typical doses, these drugs diminish the daily production of acid (basal and stimulated) by 80% to 95%. Five proton pump inhibitors are available for clinical use: omeprazole and its S-isomer esomeprazole , lansoprazole, rabeprazole, and pantoprazole.
- 19. PROTON PUMP INHIBITORS PPI are Pro-drugs - require acidic environment for activation. Activated in acidic canaliculi to sulfenamide, trapping the drug so that it cannot diffuse back across the canalicular membrane. The activated form then binds covalently with sulfhydryl groups of cysteines in the H+,K+ATPase, irreversibly inactivating the pump molecule. Acid secretion resumes only after new pump molecules are synthesized and inserted into the luminal membrane.
- 20. PROTON PUMP INHIBITORS Provides a prolonged (up to 24 - 48hrs) suppression of acid secretion, despite the much shorter plasma half-lives (0.5 - 2 hrs) of the parent compounds. Inhibit both fasting and meal-stimulated secretion because they block the final common pathway of acid secretion. In standard doses, PPIs inhibit 90–98% of 24-hour acid secretion
- 21. PROTON PUMP INHIBITORS Pharmacokinetics. Ideally should be given about 30 min before meals so that the peak serum conc coincides with the maximal activity of proton pump secretion. Rapidly absorbed in the small bowel Highly protein bound, and extensively metabolized by hepatic CYP450, particularly CYP2C19 and CYP3A4.
- 22. Clinical Comparisons of PPIs Agent Usual Dosage for Maintenance Peptic Ulcer or Therapy GERD Esomeprazole 20–40 mg qd 20 mg qd Lansoprazole 30 mg qd 15 mg qd Omeprazole 20 mg qd 20 mg qd Pantoprazole 40 mg qd 40 mg qd Rabeprazole 20 mg qd 20 mg qd
- 23. PROTON PUMP INHIBITORS Comparative Anti-secretory Efficacy of the Different PPIs Among different PPIs administered at standard doses, esomeprazole 40 mg/day has a greater anti-secretory potency Rabeprazole 20 mg/day & lansoprazole 30 mg/day show a faster action, & slightly greater acid inhibition capacity than omeprazole 20 mg/day & pantoprazole 40 mg/day
- 24. Adverse Effects Nausea, abdominal pain, constipation, flatulence Subacute myopathy, arthralgias, headaches, and skin rashes. In some patients continuously taking PPIs, a mild vitamin B12 deficiency has been seen as the result of decreased vitamin absorption due to impaired release of the vitamin from food.
- 25. ANTICHOLINERGIC DRUGS Non selectivePropantheline,Oxyphenonium. Selective M1– Pirenzepine,Telenzepine Block muscarinic M1 receptors in stomach inhibiting acid secretion. Minimal atropine like side effects on CVS,GIT or urinary bladder. Effectively heal as well as prevent the recurrence of peptic ulcer.
- 26. Prostaglandin Agonists Misoprostol (PGE1) It is a methyl analog of PGE1 Stimulate secretion of mucus & bicarbonate Binds to a prostaglandin receptor on parietal cells, reducing histamine-stimulated cAMP production and cause modest acid inhibition Stimulates intestinal electrolyte and fluid secretion, intestinal motility and uterine contractions.
- 27. Misoprostol Administration Should be given 4 time/ day Side effects Up to 20% develop diarrhea & cramps Should not be used during pregnancy.
- 28. Misoprostol Misoprostol reduces the incidence of NSAID-induced ulcers to less than 3% and the incidence of ulcer complications by 50%. It is approved for prevention of NSAIDinduced ulcers in high-risk patients.
- 29. Mucosal Protective Agents These potentiate the mucosal defensive mechanisms for the prevention and treatment of acid-peptic disorders . Sucralfate =salt of sucrose complexed to = sulfated aluminium hydroxide Forms a viscous, tenacious paste in water or acidic solutions that binds to ulcers or erosions for up to 6 hours.
- 30. Sucralfate Mechanism of action: Breaks down into sucrose sulfate (strongly negatively charged) and an aluminium salt. The negatively charged sucrose sulfate binds to positively charged proteins in the base of ulcers or erosion, forming a physical barrier that restricts further caustic damage. Stimulates mucosal prostaglandin and bicarbonate secretion. It also bind to epithelial growth factor and fibroblast growth factor, enhancing mucosal repair.
- 31. Sucralfate Administration Should not be given with food, give 1hr before or 3hr after meal Dose: 1gm/ 4times daily or 2 gm/ 2times daily Side Effects Constipation; black stool & dry mouth It is very safe in pregnancy
- 32. Colloidal Bismuth Compounds Bismuth subsalicylate Bismuth subcitrate Bismuth dinitrate
- 33. Colloidal bismuth sulfate: – Water soluble, precipitate at pH less than 5 – PG ↑ mucus secretion & bicarbonate – Forms glycoprotein complex coats ulcer – Detaches H.pylori from mucosa, kills directly – Dose = 120 mg QID
- 34. Adverse Effects Bismuth causes blackening of the stool Prolonged usage may rarely lead to bismuth toxicity resulting in encephalopathy (ataxia, headaches, confusion, seizures). High dosages of bismuth subsalicylate may lead to salicylate toxicity.
- 35. ULCER HEALING DRUGS Carbenoxolone sodium: – Steroid like derivative of glycyretenic acid found in liquorice root – Augments viscid mucus production – Prolongs life span of gastric epithelial cells, prevents bile reflux – Major problem = mineralocorticoid action so not used now a days
- 36. Antacids Weak bases that react with gastric acid to form water & salt (Neutralize acid) Also promote mucosal defense mechanisms through stimulation of mucosal PG production. A single dose of 156 meq antacid given 1 hr after meal effectively neutralize gastric acid for 2 hr.
- 37. Antacids Sodium bicarbonate reacts rapidly with HCl to produce carbondioxide and NaCl. Formation of CO2 results in gastric distention and belching. Unreacted alkali is readily absorbed, potentially causing metabolic alkalosis when given in high doses or to patients with renal insufficiency. NaCl absorption may exacerbate fluid retention in heart failure, hypertension, and renal insufficiency.
- 38. Antacids Calcium carbonate is less soluble and reacts more slowly than sodium bicarbonate with HCl to form carbon dioxide and CaCl2 Excessive doses of either sodium bicarbonate or calcium carbonate with calcium-containing dairy products can lead to hypercalcemia, renal insufficiency, and metabolic alkalosis(milk-alkali syndrome).
- 39. Antacids Magnesium hydroxide or Aluminum hydroxide react slowly with HCl to form magnesium chloride or aluminium chloride and water. No gas is generated, belching does not occur. Unabsorbed magnesium salts may cause an osmotic diarrhea and aluminium salts may cause constipation, these agents are commonly administered together.
- 40. Antibiotics for H. pylori eradication Many regimens for H. pylori eradication have been proposed. Ideal regimen in this setting should achieve a cure rate of at least 80%. Five important considerations influence the selection of an eradication regimen
- 42. Antibiotics for H. pylori eradication 1.Combination therapy with two or three antibiotics (plus acid-suppressive therapy) is associated with the highest rate of H. pylori eradication. 2. A PPI or H2-receptor antagonist significantly enhances the effectiveness of H. pylori antibiotic regimens containing amoxicillin or clarithromycin. 3. A regimen of 10 to 14 days of treatment appears to be better than shorter treatment regimens
- 43. Antibiotics for H. pylori eradication 4. Packaging that combines the daily doses into one convenient unit is available and may improve patient compliance . 5. The emergence of resistance to clarithromycin and metronidazole increasingly is recognized as an important factor in the failure to eradicate H. pylori.
- 44. Therapy of Helicobacter pylori Dual therapy (7-10 days): Omeprazole 40mg OD + Clarithromycin 500 mg TDS or Ranitidine bismuth citrate 400mg BD +Clarithromycin 500mg TDS or Omeprazole 40 mg OD +Amoxycillin 1g BD.
- 45. Therapy of Helicobacter pylori Triple therapy × 14 days: [PPI + clarithromycin 500 mg + (metronidazole 500 mg or amoxicillin 1 g)] twice a day. (Tetracycline 500 mg can be substituted for amoxicillin or metronidazole.)
- 46. Therapy of Helicobacter pylori Quadruple therapy × 14 days: PPI twice a day + metronidazole 500 mg three times daily + (bismuth subsalicylate 525 mg + tetracycline 500 mg four times daily) Or H2-receptor antagonist twice a day + (bismuth subsalicylate 525 mg + metronidazole 250 mg + tetracycline 500 mg) four times daily
- 47. Adverse Effects The most commonly reported adverse events were nausea, vomiting, & diarrhea A bitter or metallic taste in the mouth is associated with eradication regimens containing clarithromycin Bismuth subsalicylate may cause a temporary grayish-black discoloration of the stool
Hinweis der Redaktion
- has a major impact on our health care system by