Dengue algorithm
•
7 likes•6,126 views

This document provides guidance on diagnosing and managing dengue fever and its potential complications. It outlines the criteria for presumptive diagnosis of dengue and distinguishing warning signs. It then categorizes dengue cases into three groups - dengue without warning signs, dengue with warning signs, and severe dengue - with different treatment protocols depending on the severity of symptoms and laboratory findings. The treatment sections provide detailed guidance on fluid management, monitoring, and treatment of complications like shock for each dengue case category.

Recommended
More Related Content
What's hot
What's hot (20)
Viewers also liked
Viewers also liked (6)
Similar to Dengue algorithm
Similar to Dengue algorithm (20)
More from Mohd Hanafi
More from Mohd Hanafi (20)
Dengue algorithm
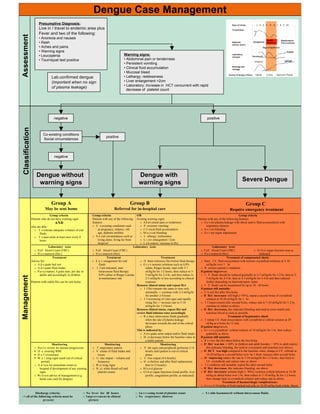
- 1. Dengue Case Management Presumptive Diagnosis: Live in / travel to endemic area plus Fever and two of the following: Assessment • Anorexia and nausea • Rash • Aches and pains • Warning signs • Leucopenia Warning signs: • Tourniquet test positive • Abdominal pain or tenderness • Persistent vomiting • Clinical fluid accumulation • Mucosal bleed Lab.confirmed dengue • Lethargy; restlessness (important when no sign • Liver enlargement >2cm • Laboratory: Increase in HCT concurrent with rapid of plasma leakage) decrease of platelet count negative positive Classification Co-existing conditions positive Social circumstances negative Dengue without Dengue with warning signs warning signs Severe Dengue Group A Group B Group C May be sent home Referred for in-hospital care Require emergency treatment Group criteria Group criteria OR Group criteria Patients who do not have warning signs Patients with any of the following Existing warning signs: Patients with any of the following features. AND features: o A b d o minal pain or tenderness o S e v ere plasma leakage with shock and/or fluid accumulation with who are able: o C o-existing conditions such o P ersistent vomiting respiratory distress o T o tolerate adequate volumes of oral as pregnancy, infancy, old o C l i nical fluid accumulation o S e v ere bleeding fluids age, diabetes mellitus o M u c o sal bleeding o S e v ere organ impairment o T o pass urine at least once every 6 o S o cial circumstances such as o L ethargy/ restlessness hours living alone, living far from o L i ver enlargement >2cm hospital o L a b oratory: increase in Hct Laboratory tests Laboratory tests Laboratory tests o Full blood Count (FBC) o Full blood Count (FBC) o Full blood Count (FBC) o O t h er organ function tests as o H a e matocrit (Hct ) o H a e matocrit (Hct) o H a e matocrit (Hct) indicated Treatment Treatment Treatment Treatment of compensated shock: Advice for: o E n c ouragement for oral o O btain reference Hct before fluid therapy o Start I.V. fluid resuscitation with isotonic crystalloid solutions at 5-10 o A d e quate bed rest fluids o G i v e isotonic solutions such as 0,9% ml/kg/hr over 1 hr o A d e quate fluid intake o I f not tolerated, start saline, Ringer lactate, start with 5-7 o R eassess patient’s condition, o P a r a c etamol, 4 gram max. per day in intravenous fluid therapy ml/kg/hr for 1-2 hours, then reduce to 3- If patient improves: adults and accordingly in children 0,9% saline or Ringer Lactate 5 ml/kg/hr for 2-4 hr, and then reduce to o I . V. fluids should be reduced gradually to 5-7 ml/kg/hr for 1-2 hr, then to 3- Management at maintenance rate 2-3 ml/kg/hr or less according to clinical 5 ml/kg/hr for 2-4 hr, then to 2-3 ml/kg/hr for 2-4 hr and then reduced Patients with stable Hct can be sent home response further depending on haemodynamic status Reassess clinical status and repeat Hct o I . V. fluids can be maintained for up to 24 - 48 hours o I f Hct remains the same or rises only If patient still unstable: minimally -> continue with 2-3 ml/kg/hr o C h eck Hct after first bolus for another 2-4 hours o If Hct increases/ still high (>50%), repeat a second bolus of crystalloid o I f worsening of vital signs and rapidly solution at 10-20 ml/kg/hr for 1 hr. rising Hct -> increase rate to 5-10 o I f improvement after second bolus, reduce rate to 7-10 ml/kg/hr for 1-2 hr, ml/kg/hr for 1-2 hours continue to reduce as above. Reassess clinical status, repeat Hct and o If Hct decreases, this indicates bleeding and need to cross-match and review fluid infusion rates accordingly transfuse blood as soon as possible o R e duce intravenous fluids gradually Treatment of hypotensive shock when the rate of plasma leakage o I nitiate I.V. fluid resuscitation with crystalloid or colloid solution at 20 decreases towards the end of the critical ml/kg as a bolus for 15 min phase. If patient im p r o v e s This is indicated by: o G i v e a crystalloid / colloid solution of 10 ml/kg/hr for 1 hr, then reduce o A d e quate urine output and/or fluid intake gradually as above o H ct decreases below the baseline value in If patient still unstable a stable patient o R e view the Hct taken before the first bolus Monitoring Monitoring Monitoring o If Hct was low (<40% in children and adult females, < 45% in adult males) o D a i l y review for disease progression: o T emperature pattern o V ital signs and peripheral perfusion (1-4 this indicates bleeding, the need to crossmatch and transfuse (see above) ! D e creasing WBC o V olume of fluid intake and hourly until patient is out of critical o If HCT was high compared to the baseline value, change to I.V. colloids at ! D e f ervescence losses phase 10-20 ml/kg as a second bolus over to 1 hour; reassess after second bolus ! W a r ning signs (until out of critical o U rine output – volume and o U rine output (4-6 hourly) o If improving reduce the rate to 7-10 ml/kgt/hr for 1-2 hours, then back to period) frequency o H ct (before and after fluid replacement, I.V. crystalloids and reduce rates as above o A d vice for immediate return to o W a r ning signs then 6-12 hourly) o I f condition still unstable, repeat Hct after second bolus hospital if development of any warning o H ct, white blood cell and o B l o o d glucose o If Hct decreases, this indicates bleeding, see above signs platelet counts o O t h er organ functions (renal profile, liver o If Hct increases/ remains high (> 50%), continue colloid infusion at 10-20 o W r i t t e n advice of management (e.g. profile, coagulation profile, as indicated) ml/kg as athird bolus over 1 hr, then reduce to 7-10 ml/kg /hr for 1-2 hours, home care card for dengue) then change back to crystalloid solution and reduce rate as above Treatment of haemorrhagic complications: o G i v e 5-10 ml/kg of fresh packed red cells or 10-20 ml/kg fresh whole blood Discharge criteria: o No fever for 48 hours o I n c r e asing trend of platelet count o S t able haematocrit without intravenous fluids -> all of the following criteria must be o Improvement in clinical o No respiratory distress present picture