Rare arterial and venous aneurysms of the gastrointestinal tract
•
0 gefällt mir•676 views

Alysha Vartevan D.O., Patricio Rossi M.D., Daryl EberM.D, Javier Casillas M.D, Beatrice Madrazo M.D. DEPARTMENT OF RADIOLOGY, LARKIN COMMUNITY HOSPITAL
Empfohlen

Empfohlen
Weitere ähnliche Inhalte
Was ist angesagt?
Was ist angesagt? (20)
Andere mochten auch
Andere mochten auch (9)
Ähnlich wie Rare arterial and venous aneurysms of the gastrointestinal tract
Ähnlich wie Rare arterial and venous aneurysms of the gastrointestinal tract (20)
Mehr von Jack Michel MD
Mehr von Jack Michel MD (16)
Kürzlich hochgeladen
Kürzlich hochgeladen (20)
Rare arterial and venous aneurysms of the gastrointestinal tract
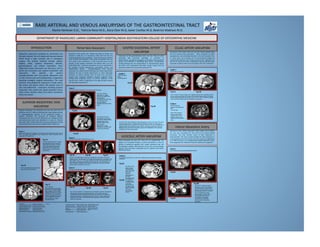
- 1. RARE ARTERIAL AND VENOUS ANEURYSMS OF THE GASTROINTESTINAL TRACT Alysha Vartevan D.O., Patricio Rossi M.D., Daryl Eber M.D, Javier Casillas M.D, Beatrice Madrazo M.D. DEPARTMENT OF RADIOLOGY, LARKIN COMMUNITY HOSPITAL/NOVA SOUTHEASTERN COLLEGE OF OSTEOPATHIC MEDICINE Splanchnic aneurysms consNtute an uncommon, but clinically relevant, form of abdominal vascular disease which shows a high mortality rate in emergency surgery. The arteries involved include: splenic, hepaNc, celiac, superior mesenteric, ileocolic, gastroduodenal, and inferior mesenteric. Intra-‐ abdominal venous aneurysms can also occur such as portal vein aneurysms and superior mesenteric vein aneurysms. The paNents can present asymptomaNcally with non-‐specific abdominal pain or with intense pain and hemodynamic compromise requiring emergent surgical intervenNon. The most common intra-‐abdominal aneurysms include aorNc, iliac artery, and splenic artery. We present cases of rare intra-‐abdominal aneurysms including superior mesenteric vein, portal vein, gastro-‐duodenal artery, celiac artery, ileocolic artery and inferior mesenteric artery aneurysms. INTRODUCTION Superior mesenteric vein aneurysms are very rare with only 10 published cases (1). PaNents presented with vague abdominal pain or asymptomaNcally. Because of the anatomical locaNon, a superior mesenteric vein aneurysm can compress adjacent extrahepaNc bile ducts and the duodenum (2). Elevated bilirubin and transaminase levels were described in 2 cases (1). Theories about the origin of these aneurysms have been proposed including local inflammatory processes and congenital abnormaliNes (2). SUPERIOR MESENTERIC VEIN ANEURYSM Case 1: 55-year-old female with cryptogenic cirrhosis and portal hypertension that required TIPS. The patient was referred to our institution for further evaluation due to suspected TIPS malfunction. Fig 1A Fig 1B Fig 1C Aneurysms of the gastroduodenal artery are rare. They are o_en associated with pancreaNc pathology or secondary to atherosclerosis. Computed tomography and Doppler ultrasound have shown to be effecNve in idenNfying these lesions. ComplicaNons include bleeding into the intraperitoneal or retroperitoneal spaces (4). Other rare complicaNons described include rupture into the portal vein and/or into a pancreaNc pseudocyst (5). GASTRO-‐DUODENAL ARTERY ANEURYSM CASE 5: Fig 5A Fig 5B These aneurysms are also rare. They can be asymptomaNc and appear as an incidental finding on rouNne examinaNon or they can present as abdominal apoplexy with sudden abdominal pain and hemodynamic collapse. Atherosclerosis is the most common eNology, however they have been incidentally found in paNents with Ehlers-‐ Danlos and Lupus. ILEOCOLIC ARTERY ANEURYSM Fig. 6A-B: CECT shows a large heterogeneous mass in the right side of the abdomen, anterolateral to the aorta (arrowhead) with the epicenter in the mesentery. Fig 6A Fig 6B Aneurysms of the celiac artery are rare and include approximately 4% of all visceral artery aneurysms. These aneurysms are o_en asymptomaNc and incidentally detected in the sixth decade of life. In recent years, the increased use of cross-‐secNonal imaging has improved the detecNon rate of these aneurysms (6). Although rare, the risk of rupture and other complicaNons warrant elecNve repair, especially in paNents with aneurysms greater than two cenNmeters. CELIAC ARTERY ANEURYSM CASE 7: Celiac Artery Aneurysms CASE 8: Fig. 7A: Plain CT shows a large, oval, irregular structure with a calcified wall (red arrow) located anterolateral to the aorta (arrowhead). Note the areas of increase density representing acute bleed (blue arrow). Fig. 7B: CECT shows the irregular lumen and demonstrates active extravasation (arrowheads). Fig 7A Fig 7B Fig 8: CECT shows a fusiform celiac artery aneurysm of 2.0 cm in diameter (black arrow). Patient was post-op AAA repair. Aneurysms of the Inferior Mesenteric Artery (IMA), Arch of Riolan, are very rare, accounNng for only 0.5% of all visceral arterial aneurysms. The most common cause of these aneurysms is atherosclerosis. The most common locaNon for these aneurysms is in the proximal trunk of the artery. The most common manifestaNon of an IMA aneurysm is an asymptomaNc pulsaNle abdominal mass. Once diagnosed, the method of choice for treatment is surgical(7). Inferior Mesenteric Artery Case 9: Arch of Riolan Aneurysm and Polyarteritis Nodosa Fig 9A Fig 9B Fig 9C Aneurysm of the portal vein, iniNally described by Barzilai and Kleckner in 1956 (3), is an uncommon enNty with less than one hundred published cases worldwide. These aneurysms are defined by an increase focal diameter of the portal vein greater than one and a half to two cenNmeters. It most commonly occurs at the juncNon of the superior mesenteric and splenic veins or at the portal bifurcaNon. Portal vein aneurysms can occur secondarily in the seings of portal hypertension, pancreaNNs, trauma, and hepatocellular disease. Histopathologically, these acquired aneurysms can exhibit inNmal thickening and medial hypertrophy. However, the lack of portal hypertension or other pathologic processes in several reported cases of portal vein aneurysms support other proposed eNologies including congenital origin. Among these congenital causes, an intrinsic weakness of the vascular wall or failure of regression of the right primiNve vitelline vein have been proposed (2). Portal Vein Aneurysm Case 2: 51-year-old male complaining of non-specific abdominal pain Case 3: 45-year-old male with incidental finding on US Case 4: 48-year-old female, complaining of right upper quadrant pain Fig. 2A-B: Contrast enhanced CT images through the hepatic hilum demonstrate a homogeneously enhancing round structure with markedly different diameters at the two shown levels. Fig. 3A: CT image shows a large oval hypodensity in the region of the porta hepatis (arrow). Fig. 3B: Axial T1-W image demonstrates flow void signal in the same region. Fig. 3C: T2-W Fat Sat. sequence shows focal hyperintensity with flow void in the periphery compatible with turbulent flow. The combination of these findings is consistent with a portal vein aneurysm. Note the incidental simple cysts in the left lobe of the liver. Fig. 4A: Non contrast T1-W shows focal oval dilatation with flow void signal at the junction of the main and right portal veins. In Fig. 4B this structure demonstrates strong homogeneous enhancement identical to the adjacent portal vein branches. Gray scale US shown in Fig. 4C : again confirms the presence of the lesion. These findings were diagnostic of a proximal right portal vein aneurysm. Fig 2A Fig 2B Fig 3A Fig 3B Fig 3C Fig 4A Fig 4B Fig 4C REFERENCES: 1- Wolosker N, Zerati, et al. Aneurysm of Superior Mesenteric Vein: Case report with a 5 year follow-up and review of the literature. J Vascular Surgery 2004; 39: 459-461. 2- Furcher A. and Turner M. Aneurysms of the portal vein and superior mesenteric vein. Abdominal Imaging 1997; 22: 287-292. 3- Barzilai R. and Kleckner M.S. Jr. Hemocholecyst following ruptured aneurysm of portal vein. Archives of Surgery 1956; 72: 725-727. 4- Jamal HZ, and KP Block. Endoscopic appearance of gastroduodenal artery aneurysm. Gastrointestinal Endoscopy 1999; 50:862-863. Contrast enhanced axial CT image demonstrates the stent inside the main portal vein (arrow), note the numerous collaterals around the right portal vein consistent with partial cavernous transformation (arrowhead). CECT demonstrates the stent at the level of the portal confluence. CECT shows a pseudoaneurysm of the SMV (blue arrow). Findings suggest stent migration due to venous dilatation secondary to venous hypertension and subsequent intimal hyperplasia around the proximal aspect of the stent with formation of a distal pseudoaneurysm. Fg. 5A-B: CECT demonstrating a large heterogeneous mass in the area of the head of the pancreas (arrow). The lesion extends inferiorly and there is a focal area of intense enhancement consistent with a vascular structure. This was consistent with a gastroduodenal artery pseudoaneurysm within a pancreatic pseudocyst. Note the dilatation of the pancreatic duct and the presence of calcifications in the pancreas consistent with chronic pancreatitis CASE 6: Young patient with history of Lupus (SLE), diiffuse abdominal pain and dropping hematocrit This vascular structure corresponds to the portal vein (arrow). Note the distal dilatation with normal proximal caliber and no signs of portal hypertension. These findings are consistent with a portal vein aneurysm. In addition there is free fluid around the liver and diffuse high signal consistent with active extravasation (arrow) Fig. 9A-B: CT without contrast showing an area of high density in the left mesentery and left lower quadrant with small amount of free fluid (arrows). Fig. 9C: T1-W Fat. Sat. post gadolinium image demonstrates a central round hyperintense mass (arrow) surrounded by low signal representing a mesenteric aneurysm with surrounding hematoma. 5- Yeh TS, Jan YY, Jeng LB, et al. Massive extra-enteric gastrointestinal hemorrhage secondary to splanchnic artery aneurysms. Hepatogastroenterology 1997; 44:1152-1156. 6- Soudack M, Gaitini D, and Ofner A. Celiac artery aneurysm: diagnosis by color Doppler sonography and three- dimensional CT angiography. J Clin Ultrasound 1999; 27:49-51. 7Davidovic Lazar B, Vasic Dragan M, and Colic Momcilo I. Inferior Mesenteric Artery Aneurysm: Case Report and Review of Literature. Asian J of Surgery 2003; 26 (6); 176-179. CASES PRESENTED FROM LARKIN COMMUNITY HOSPITAL, HEALTH CARE IMAGING, AND JACKSON HOSPITAL UNIVERSITY OF MIAMI Gastro-Duodenal Artery Pseudoaneurysm 58-year-old male presents with abdominal pain s/p AAA stent