Metastatic renal cell carcinoma presenting as a thyroid nodule
•
0 gefällt mir•726 views

Joshua Simon, DO, PGY-1, Philip Pack, DO, PGY-2, Quoc Dang, DO, PGY-1, Michael Kambour, MD, and Mohammad Masri, MD Larkin Community Hospital General Surgery Residency Program

Empfohlen
Weitere ähnliche Inhalte
Was ist angesagt?
Was ist angesagt? (20)
Ähnlich wie Metastatic renal cell carcinoma presenting as a thyroid nodule
Ähnlich wie Metastatic renal cell carcinoma presenting as a thyroid nodule (20)
Mehr von Jack Michel MD
Mehr von Jack Michel MD (17)
Kürzlich hochgeladen
Kürzlich hochgeladen (20)
Metastatic renal cell carcinoma presenting as a thyroid nodule
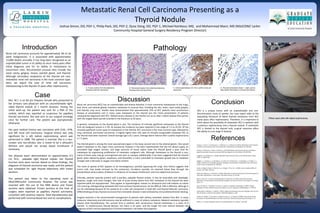
- 1. Renal cell carcinoma accounts for approximately 3% of all adult malignancies. It is associated with approximately 13,000 deaths annually. It has long been recognized as an unpredictable tumor in its ability to recur many years after initial diagnosis and for its ability to metastasize to uncommon sites. Documented unusual sites include the nasal cavity, gingiva, larynx, parotid gland, and thyroid. Although secondary neoplasms of the thyroid are rare, metastatic renal cell carcinoma is the most common type. Here, we report the case of renal cell carcinoma metastasizing to the thyroid 15 years after nephrectomy. Conclusion Pathology References Renal cell carcinoma (RCC) has an unpredictable and diverse behavior. It most commonly metastasizes to the lungs, liver, bone, and adrenal glands; however, metastasis to unusual sites, including the skin, testis, nasal cavity, gingiva, and thyroid, may occur. Studies have demonstrated that approximately 25% of RCC patients have synchronous disease at presentation and in many cases metastasis to the thyroid was the initial presentation of patients subsequently diagnosed with RCC. Metachronous disease to the thyroid can occur after a latent disease-free period, with the longest latent period recorded in the literature as 26 years. In general, metastases to the thyroid gland is rare. The incidence of clinically significant metastases to the thyroid from all malignant tumors is 2-3%. At autopsy the incidence has been reported in the range of 1.2 to 24.2%. Of the clinically significant tumor types to metastasize to the thyroid, RCC carcinoma is the most common type, followed by lung, colorectal, and breast carcinomas. A slightly higher than 150 cases of clinically recognizable metastatic RCC to the thyroid have been reported. Overall average age is 62.1 years. Average latent interval after curative nephrectomy is 7.5 years. The thyroid gland is among the most vascularized organs in the body, second only to the adrenal glands. One would expect metastasis to this organ more commonly, however it has been hypothesized that the rich blood supply, an associated high oxygen tension, and large amounts of tissue iodine make the thyroid gland a poor host for metastases by suppressing proliferation of metastatic malignant cells. Although metastases to the thyroid is rare, many of these cases may go unrecognized and seen on autopsy. Additionally, it has been suggested that the thyroid gland, when altered by goiter, neoplasms, and thyroiditis, is more vulnerable to metastatic growth due to metabolic changes with a decrease in oxygen and iodine content. The route of spread of RCC appears to be hematogenous, possibly bypassing the lungs. One theory suggests that tumor cells may evade removal by the pulmonary circulation possibly via reversed blood flow through the paravertebral venous plexus of Batson in situations of increased intrathoracic and intra-abdominal pressure. Clinically, patients typically present with a painless, palpable thyroid nodule. It may be associated with dysphagia, dyspnea, cough, and vocal changes. One case of acute airway failure from RCC metastasis to the thyroid has been reported while are asymptomatic. They appear as hypoechogenic masses on ultrasound and cold nodules on iodine 131 scanning. Distinguishing metastatic RCC from primary thyroid tumors can be difficult. FNA is effective, although it can be misleading because of the presence of a clear cell component in both RCC and thyroid follicular carcinoma. Differentiating primary thyroid carcinoma from metastatic disease is best achieved by immunohistochemical staining. Surgical resection is the recommended management of patients with solitary metastatic disease from RCC. In many instances, lobectomy and isthmectomy may be sufficient in cases of solitary metastasis. Bilateral metastasis typically require total thyroidectomy. The survival time in patients with synchronous thyroid metastases is a mean of 8 months. In metachronous thyroid disease, the mean is 10 years, and the longer the time interval between the diagnosis of RCC and the appearance of thyroid metastasis, the better the prognosis. Introduction Discussion A Case Mrs. M.J. is an 84 y/o Hispanic female who presented to her primary care physician with an uncomfortable right- sided thyroid nodule of 1 month duration. During the initial work-up, the patient was sent for a FNA of the nodule, which was reported as suspicious for papillary thyroid carcinoma. She was sent to our surgical oncology clinic for further care. The patient was asymptomatic otherwise. Her past medical history was consistent with D.M., HTN, and left renal cell carcinoma. Surgical history was only significant for a left radical nephrectomy, which was performed in 1998. The patient is married. She is a non- smoker and non-drinker. She is noted to be a Jehovah’s Witness and would not accept blood transfusion if necessary. Her physical exam demonstrated an approximately 0.5 cm, firm, palpable right thyroid nodule. Her thyroid function tests were normal. Based on these findings, the diagnosis of thyroid carcinoma was made, and the patient was scheduled for right thyroid lobectomy with frozen sections. The patient was taken to the operating room at NSUCOM/Larkin Community Hospital. The tumor was resected with the use of the NIM device and frozen sections were obtained. Frozen sections at the time of surgery were reported as papillary thyroid carcinoma, consistent with previous reports. Total thyroidectomy was performed with minimal blood loss and no complications. Chung, A., Y, Tran, T., B, Brumund, K., T, Weisman, R., A, Bouvet, M. (2012). Metastases to the Thyroid: A Review of the Literature from the Last Decade. Thyroid Cancer and Nodules, 22, 258-268. Di Stasi, V, D’Antonio, A, Caleo, A, Valvano, L. (2013) Metastatic renal cell carcinoma to the thyroid gland 24 years after the primary tumour. BMJ Case Reports. doi:10.1136/bcr-2012-007569 Duggal N., M, Horattas M., C. (2008). Metastatic Renal Cell Carcinoma to the Thyroid Gland. Endocr Pract, 14, 1040-1046. Hughes, J., H, Jensen, C., S, Donnelly, A., D, Cohen, M., B, Silverman, J., F, Gelsinger, K., R, Raab, S., S. (1999). The Role of Fine-Needle Aspiration Cytology in the Evaluation of Metastatic Clear Cell Tumors. Cancer (Cancer Cytopathol), 87, 380-389. Jemal, A, Siegel, R, Ward, E, Murray T, Xu, J, Smigal, C, Thun, M., J. (2006). Cancer statistics 2006. CA Cancer J Clin, 56(2), 106-130. Kihara, M, Yokomise, H, Yamauchi, A. (2004). Metastasis of renal cell carcinoma to the thyroid gland 19 years after nephrectomy: a case report. Auris Nasus Larynx, 31, 95-100. Riaz, K, Tunio, M., A, Al Asiri, M, Mohammad, A, Fareed, M., M. (2013). Renal Cell Carcinoma Metastatic to Thyroid Gland, Presenting Like Anaplastic Carcinoma of Thyroid. Case Reports in Urology, 2013, 1-4. Rizzo, M, Rossi, R., T, Bonaffini, O, Scisca, C, Sindoni, A, Altavilla, G, Benvenga, S. (2009). Thyroid Metastasis of Clear Cell Renal Carcinoma: Report of a Case. Diagnostic Cytopathology, 37, 759-762. Sountoulides, P, Metaxa, L, Cindolo, L. (2011). Atypical presentations and rare metastatic sites of renal cell carcinoma: a review of case reports. J Med Case Reports, 5, 429. Testini, M, Lissidini, G, Gurrado, A, Lastilla, G, Ianora, A., S, Fiorella, R. (2008). Acute Airway Failure Secondary to Thyroid Metastasis from Renal Carcinoma. World Journal of Surgical Oncology, 6, 14. Willis, R., A. (1931). Metastatic tumors in the thyroid gland. Am J Pathol, 7, 187-208. Metastatic Renal Cell Carcinoma Presenting as a Thyroid Nodule Joshua Simon, DO, PGY-1, Philip Pack, DO, PGY-2, Quoc Dang, DO, PGY-1, Michael Kambour, MD, and Mohammad Masri, MD (NSUCOM/ Larkin Community Hospital General Surgery Residency Program Director) C. Immunoperoxidase CD-10 to confirm renal cell carcinoma. B. Permanent section from total thyroidectomy showing renal cell carcinoma. A. Frozen section from thyroidectomy showing renal cell carcinoma. D. Thyroid transcription factor -1 stain used to help confirm the tissue is not from the thyroid. Fifteen years after left radical nephrectomy. Two weeks after total thyroidectomy. RCC is a unique tumor with an unpredictable and non- discriminatory route of spread. Our case report adds to the expanding literature of latent thyroid metastasis from RCC many years after nephrectomy. Therefore, it is important to think about the possibility of metastatic RCC in patients with a previous nephrectomy and a thyroid nodule. If metastatic RCC is limited to the thyroid only, surgical resection offers the ability to cure stage IV disease.