
Empfohlen
Weitere ähnliche Inhalte
Was ist angesagt?
Was ist angesagt? (17)
Andere mochten auch
Andere mochten auch (10)
Ähnlich wie Judd Young Poster - Robinson, Herbert, Afari, and Wetherell
Ähnlich wie Judd Young Poster - Robinson, Herbert, Afari, and Wetherell (20)
Judd Young Poster - Robinson, Herbert, Afari, and Wetherell
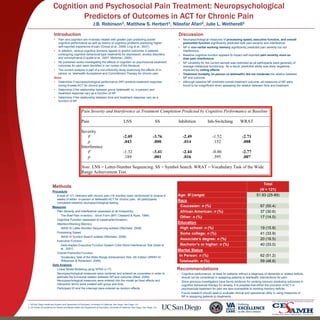
- 1. Cognition and Psychosocial Pain Treatment: Neuropsychological Predictors of Outcomes in ACT for Chronic Pain J.B. Robinson1, Matthew S. Herbert1, Niloofar Afari2, Julie L. Wetherell1 Introduction • Pain and cognition are inversely related with greater pain predicting poorer cognitive performance as well as history of cognitive problems predicting higher self-reported experience of pain (Grossi et al., 2008; Ling et al., 2007). • In addition, various cognitive domains appear to predict outcomes in patients undergoing cognitive-behavioral type treatments for depression, anxiety disorders, and schizophrenia (Caudle et al., 2007; Mohlman, 2005). • No published works investigating the effects of cognition on psychosocial treatment outcomes for pain were identified in our review of the literature. • The current analysis is part of a non-inferiority study examining the effects of in- person vs. telehealth Acceptance and Committment Therapy for chronic pain. Aims: • Determine if neuropsychological performance (NP) predicts treatment response during 8-week ACT for chronic pain • Determine if the relationship between group (telehealth vs. in-person) and treatment response vary as a function of NP • Determine if the relationship between time and treatment response vary as a function of NP 1. VA San Diego Healthcare System and Department of Psychiatry, University of California, San Diego, San Diego, CA. 2. VA Center of Excellence for Stress and Mental Health and Department of Psychiatry, University of California, San Diego, San Diego, CA Methods Procedure: A total of 121 Veterans with chronic pain (>6 months) were randomized to receive 8 weeks of either in-person or telehealth ACT for chronic pain. All participants completed baseline neuropsychological testing. Measures: Pain Severity and Interference (assessed at all timepoints): The Brief Pain Inventory - Short Form (BPI; Cleeland & Ryan, 1994) Cognitive Function (assessed at baseline/termination): Attention/Working Memory WAIS-IV Letter-Number Sequencing subtest (Wechsler, 2008) Processing Speed WAIS-IV Symbol Search subtest (Wechsler, 2008) Executive Function Delis-Kaplan Executive Function System Color-Word Interference Test (Delis et al., 2001) Overall Premorbid Function Vocabulary Task of the Wide Range Achievement Test, 4th Edition (WRAT-IV, Wilkenson & Robertson, 2006) Data Analysis: Linear Mixed Modeling using SPSS (v.17) Neuropsychological measures were centered and entered as covariates in order to estimate the functional relation between NP and outcome (West, 2009). Neuropsychological measures were entered into the model as fixed effects and interaction terms were created with group and time. Participant ID and the intercept were entered as random effects. Recommendations • Cognitive performance, at least for patients without a diagnosis of dementia or related deficits, should not be considered in assigning patients to telehealth interventions for pain. • Since previous investigators have found evidence for working memory predicting outcomes in cognitive behavioral therapy for anxiety, it is possible that either the provision of ACT or psychosocial treatment for pain are less susceptible to working memory deficits. • Future research should seek to evaluate clinical and operational utility in using measures of NP in assigning patients to treatments Total (N = 121) Age: M (range) 51.93 (25-89) Race Caucasian: n (%) 67 (55.4) African American: n (%) 37 (30.6) Other: n (%) 17 (14.0) Education High school: n (%) 19 (15.8) Some college: n (%) 41 (33.9) Associate’s degree: n (%) 20 (16.5) Bachelor’s or higher: n (%) 40 (33.0) Marital Status In Person: n (%) 62 (51.2) Telehealth: n (%) 59 (48.8) Discussion • Neuropsychological measures of processing speed, executive function, and overall premorbid function significantly predicted both pain severity and interference. • NP in non-verbal working memory significantly predicted pain severity but not interference. • Baseline cognitive function appears to impact self-reported pain severity more so than pain interference. • NP variability for the current sample was restricted as all participants were generally of average intellectual functioning. As a result, predictive ability was likely negatively impacted by ceiling effects. • Treatment modality (in-person vs telehealth) did not moderate the relation between NP and outcome. • Although baseline NP predicted overall treatment outcome, all measures of NP were found to be insignificant when assessing the relation between time and treatment. Pain Severity and Interference at Treatment Completion Predicted by Cognitive Performance at Baseline Pain LNS SS Inhibition Inh-Switching WRAT Severity F -2.05 -3.76 -2.49 -1.52 -2.71 p .043 .000 .014 .132 .008 Interference F -1.32 -3.41 -2.44 -0.86 -2.77 p .189 .001 .016 .395 .007 Note. LNS = Letter-Number Sequencing. SS = Symbol Search. WRAT = Vocabulary Task of the Wide Range Achievement Test.