1. SUNDAYT H E P R O V I N C E . C O M
AUGUST 26, 2012
$2.90 minimum
in outlying areas
$2.25PLUS
HST
FINAL EDITION
A DIVISION OF
POSTMEDIA NETWORK INC.
II
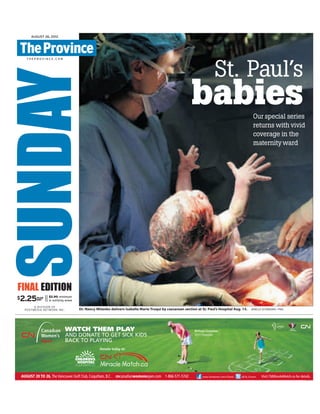
Dr. Nancy Mitenko delivers Isabella Marie Truqui by caesarean section at St. Paul’s Hospital Aug. 15. JENELLE SCHNEIDER / PNG
St. Paul’s
babiesOur special series
returns with vivid
coverage in the
maternityward
VAN01098101_1_1
2. beatheart
Inside St. Paul’s
Hospital
Oneminutetheyareone.
In an instant, there are
two.Thesuddencleav-
ing of baby from mother in the
operating room is shocking
and sudden, both frightening
and beautiful.
As the doctor lifts the baby
aloftandeveryoneturnstosee
her,foraheartbeat,itfeelslike
no one in the room is breath-
ing. That is the split-second
magic of a surgical caesarean-
section delivery.
Then the spell is broken as
the little girl fills her lungs and
withherfirstcryexclaims:“I’m
here!”
“Happy birthday, girl, wel-
come to the world,” coos a
nurseassherubsthenewchild
with a cloth.
Her mother, Lorena Truqui,
lies back quietly beyond a
drape, unable to witness this
birth. But tears slip out of the
sides of her eyes as she listens
to her baby.
“I’m so happy,” she tells
her husband, Juan, who has
been at her side soothing her
through the surgery.
“We’re so blessed,” he tells
her, lovingly.
When her just-born seven-
pound girl is brought to her
minutes later and laid on her
chest, the tears fall faster.
“Hi, sweetie. Don’t cry, my
baby,” her mother whispers,
gazing at her daughter.
Isabella Marie reaches out
a tiny hand, opens her eyes
and then instinctively tries to
suckle, hungry for life as well
as food.
■
More than 1,660 babies were
born at St. Paul’s Hospital last
year.Manyofthem,likeIsabel-
la,tooktheirfirstbreathsinthe
operating room.
That’s because St. Paul’s,
unlike other community hos-
pitals, is a centre for treating
anddeliveringthehighest-risk
mothersintheprovince.These
complex cases can involve
heart and kidney disease or
multiple medical conditions
and often require surgical
deliveryforthehealthofmoth-
er and baby.
But those factors aside,
C-sectiondeliveriesareonthe
rise worldwide. The medical-
izationofbirthisafactofmod-
ern medicine.
Last year, more than 371,000
babies were born in Canadi-
an hospitals, according to the
Canadian Institute for Health
Information.About18percent
of Canadian women birthing
for the first time in 2011 had
C-sections. In the 1960s, the
rate was just five per cent.
B.C. has among the highest
primary C-section rates in the
country,at23percent.Among
B.C. women 35 and older, that
figure jumps to more than 28
per cent.
At St. Paul’s, the C-section
rate is higher still.
‘Welcome
to the world’
Safe in the hands of Dr. Nancy Mitenko, Isabella Marie Truqui makes her debut in the world after a caesarean section
was performed on her mother, Lorena Truqui. PHOTOS BY JENELLE SCHNEIDER — PNG
A fierce and
beautiful love
If you want proof of the extraor-
dinary lengths to which women
will go to bring new life into the
world, spend a week in a mater-
nity ward. Here, a steady stream
of women brave pain and illness,
endure weeks of bedrest and diag-
nostic tests, and undergo sur-
gery and sleepless nights — all
to birth their babies safely. They
may end up in intensive care, in
the operating room or have their
newborns sent to intensive care.
But they get through it, drawing
strength from a fierce and beauti-
ful love for a child they have nev-
er met. And every time it gets hard,
the staff of St. Paul’s Hospital are
there: holding their hands, calm-
ing their fears, coaching them
through labour and treating com-
plicated conditions with stunning
expertise. It’s hard work over long
hours, but staff say their job has
its own rewards. Every day, they
bear witness to that perfect, sacred
moment of birth — the stunning
split-second when a baby takes a
breath and announces itself to the
world.
This week, The Province brings
you the intimate stories of new
families created at St. Paul’s and
of the dedicated care that makes
it possible, sometimes against all
odds.
Thisweek:
Thematernityward
Heartbeat is an eight-month special series for which The Province has been granted
special access to St. Paul’s Hospital. The series runs for a week each month until November.
A12 SUNDAY, AUGUST 26, 2012| SPECIAL SERIES | THEPROVINCE.COM
Elaine O’Connor
SUNDAY
REPORTER
eoconnor@
theprovince.com
twitter.com/
elainereporting
theprov.in/
bcwithoutborders
3. In 2011-12, it was 40.3 per cent
forallmothers.Thehospital’spri-
maryC-sectionrate—theelective
procedures of first-time mothers
— for that period is 27.4 per cent.
Butthosehighnumbersbeliethe
unusualcomplexityofmanyofSt.
Paul’smaternitypatients,explains
Dr.ElisabetJoa,headofobstetrics
and gynecology for Providence
HealthCareandchairofSt.Paul’s
renal obstetric clinic.
“It’s higher than most hospi-
tals because we take care of the
really critical-care mothers,” she
stresses.
Also,womennowarebecoming
mothers later and using in-vitro
fertilization methods more fre-
quently, so that maternal age and
multiple births are other contrib-
uting factors to C-section rates.
“As women get older, unfortu-
nately, we labour differently and
not as successfully,” says Joa, who
delivered three of her own five
children at St. Paul’s.
St. Paul’s also offers elective
C-sections — not all hospitals do
— and some women, even when
theyknowthatC-sectionsinvolve
higherrisktothemotherthanvag-
inal deliveries and can result in
complications such as infection
and hemorrhaging, will choose
to go under the knife for person-
al or cultural reasons.
C-sectionscanberiskyforbaby,
too: without the aid of pressure
from labour, their lungs retain
water and often don’t function as
well at birth.
Critics and advocates of natural
childbirth often lay the blame for
high C-section rates on the over-
use of interventions early on in
labour, namely, premature med-
ical induction of labour and the
use of oxytocin to augment con-
tractions, which can stress the
fetus. Obsessive monitoring of
fetal heart rate and the resulting
impeded ability of a woman to
move during labour is also cited,
as is the use of epidurals — pain-
killing spinal injections — which
often stall labour progress.
■
In Lorena’s case, she’s at St.
Paul’s because she’d previously
had C-sections for medical rea-
sons and thought it prudent to do
so again with her third.
Her choice is one most mothers
in her situation make. Although
vaginal birth after caesarean sec-
tion (VBAC) is possible, the over-
allrepeatC-sectionrateinCanada
isanastonishing82percent,with
B.C. just slightly under the aver-
age.It’sclearthatinmanyofthese
casespatientsandphysicianspre-
fer or feel it safer to deliver surgi-
cally.
Lorena had few reservations,
and as she lay in the surgical day-
careunitwaitingherturn,shewas
morefocusedontheendthanthe
means of her daughter’s birth.
“I just kept dreaming all night
about holding the baby.”
Herhusbandwasmorecautious.
“I’m not nervous, but it’s quite an
operation. It’s done every day,
thousands of times a day, but it’s
still major surgery.”
However their daughter came
intotheworld,onceshewasthere,
it was not the surgery on her par-
ents’ mind, but celebration.
The next afternoon, there is a
party in room 20.
The Truquis’ two children are
there to see their newest sibling,
as are two grandparents who’ve
come all the way from Mexico to
meet their ninth grandchild.
The children plaster the room
with hand-drawn welcome signs
that read: “Welcome Bebe.”
“We used to be just four, so it’s
weird to be five,” Anna Paula, 8,
says thoughtfully.
The siblings waste little time
squabbling affectionately over
their newest addition.
“I’m going to burp her,” Anna
says proudly.
“I’mgoingtochangeherdiaper,”
chimes her younger brother, Ian,
perhaps not fully understanding
what he’s in for.
“I’m going to teach her to walk,”
Anna one-ups him.
“I’m going to teach her how to
do the monkey bars,” he shoots
back.
Lorena and Juan smile indul-
gently.
One day Isabella, too, will have
to learn to find her own place in
their family. But for now, swad-
dled and sleeping on her moth-
er’s chest, she’s simply the quiet
centre of it all.
Juan and Lorena Truqui with daughter Ana Paula, son Ian Paul and the newly arrived Isabella Marie
Truqui in the maternity ward of St. Paul’s.
onlinetheprovince.com/heartbeat
Photos videos your feedback
See more stunning photos of
Isabella’s C-section birth
Activity in the St. Paul’s
maternity ward during
the week of TheProv-
ince’s visit Aug. 13-17:
Monday
Total births: 7
C-sections: 4
Boys: 2
Girls: 5
Tuesday
Total births: 5
C-sections: 2
Boys: 4
Girls: 1
Wednesday
Total Births: 7
C-sections: 5
Boys: 3
Girls: 4
Thursday
Total births: 7
C-sections: 3
Boys: 2
Girls: 5
Friday
Total births: 5
C-sections: 1
Boys: 3
Girls: 2
Baby boom
Dr. Elisabet Joa says the C-section rate at St. Paul’s reflects
the high percentage of critical-care pregnancies the
hospital takes on.
SUNDAY, AUGUST 26, 2012 A13| THEPROVINCE.COM | SPECIAL SERIES |
4. It was June of 1961. My mother was
very pregnant with me. My dad was out
of town working as a boilermaker.
A week before I was due, my mother
went into labour. My sister was dropped
off at a neighbour’s house and a friend
took my mother to St. Paul’s Hospital. I
was a breech case and it was a difficult
labour. As my mom was trying to deliver,
she went into cardiac arrest.
When the hospital finally reached my
dad, they told him on the phone they
had called the priest in and were not
sure if she would make it through the
night. My dad got to the hospital as soon
as he could.
Luckily for my mother, she was at St.
Paul’s Hospital.They opened up her
chest while I was being born and mas-
saged her heart.They got it started and
delivered me at the same time.That was
on June 7, 1961. My mom survived and
eventually was able to bring me home.
Needless to say, there are no baby pic-
tures of me.
My formula recipe that the nurses gave
my mother was Carnation evaporated
milk diluted with water and with a tea-
spoon of sugar added.
My mom died of cancer in 1985. I am so
happy I was able to have 56 years with
my mother. If it wasn’t for the doctors at
St Paul’s Hospital, I don’t think she would
have made it.
My husband’s mother was also born
at St Paul’s. Of course, both my children
were born there, too: my daughter Emily
in 1997 and my son Dane in 1999.
Thank you, St. Paul’s Hospital, from
three generations of babies.
— Diana Fiola, Vancouver
Diana Fiola, at about 10 months, with
her mother, Irene Charun.
By Elaine O’Connor
THE PROVINCE
It’s a strange place for a baby to
sleep — in a bassinet hidden in a
cupboard at a busy ambulance
entrance.
But the Angel’s Cradle at St.
Paul’s isn’t meant to offer infants
sweet dreams, rather to give des-
peratemothers asafe place toact
on the heart-wrenching decision
to give up their babies.
The program was launched
in May 2010 at the urging of Dr.
Geoffrey Cundiff, then the hospi-
tal’s head of obstetrics and gyne-
cology, the field he now oversees
fortheVancouverCoastalHealth
region. He’d been troubled by
news reports of a mother who’d
abandoned her dead newborn.
Surely, he thought, there must be
a way to help women who are too
distraught to give their children
up through traditional methods
such as adoption.
Herecalledthefoundlingwheels
usedinthe12thcenturytoaccept
unwantedbabiesandthoughtthe
idea a good match for St. Paul’s
mission of compassionate care.
“It was a good opportunity to
reach women in crisis,” Dr. Cun-
diffsaid.“Thereareotheroptions
out there, but the difference with
this is it allows for anonymity.”
At least one mother agreed.
Because just months after the
Angel’s Cradle opened, one
afternoon in mid-July, someone
opened the door on the outside
ofthehospitalandplacedadays-
oldbabyboysafelyinsidethebas-
sinet, leaving him to his new life.
A minute later, an alert rang out
in the emergency department.
Nurse Kirsten Fuller thought it
wasjustanotherfalsealarm.Para-
medics had been known to open
thedooroutofcuriosity.Butwhen
sheandaco-workerlookedinthe
cupboard, they got a shock.
“There was this beautiful, per-
fect baby boy,” Fuller recalled.
With the baby were bottles, dia-
pers and notes about his birth
date, health and background.
“If you had wanted to trace that
child, it would have been easy
withtheinformationtheyhadgiv-
enus,”Fullersaid.“Butourpolicy
is not to trace them.”
Indeed, Vancouver police have
assured hospital staff they will
not attempt to locate parents of
Angel’s Cradle babies. In Cana-
da, child abandonment is only a
criminaloffenceifthechildisleft
alone in a way that causes inju-
ry or endangers its health. The
purpose of the Angel’s Cradle
— unique in the country — is to
ensure the child’s safety.
“For whatever reason, they
couldn’t look after this child,”
Fuller said. “This was their safe
place to drop him off. But clear-
ly, he was loved.”
Thechildwasquicklyexamined
by paramedics, then taken to the
neonatalintensivecareunit.Staff
camefromallovertogetaglimpse
of the foundling.
“Itwasawholemixofemotions,”
Fullerrecalled.“Wewerehappya
baby had got dropped off healthy
that might have otherwise been
neglected.Weweresadthatbaby
was now going into foster care.”
Severaltroublingcasesofinfan-
ticide and child abandonment
have also made headlines in the
province.ButwhileSt.Paul’sstaff
know they can’t protect every
child,they’regladthey’vehelped
at least one.
“It can’t save every baby,” Dr.
Cundiff said, “but my hope is this
will give us a way to save some.”
eoconnor@theprovince.com
The day an angel came calling
Kirsten Fuller was one of two nurses who found the Angel’s Cradle baby at St. Paul’s Hospital in 2010. The cradle has a door that
can be opened from the outside and is located at the emergency department entrance. JENELLE SCHNEIDER — PNG
Your memories
Do you have a St. Paul’s story? Submit it at
theprovince.com/stpaulsstories
HEARTBEAT CONTINUES TOMORROW
beatheart
Inside St. Paul’s
Hospital
Heart stopped
while baby
was en route
“For whatever reason, they couldn’t look
after this child. This was their safe place to
drop him off. But clearly, he was loved.”
KIRSTEN FULLER—
ST. PAUL’S NURSE
“It can’t save every
baby, but my hope
is this will give
us a way to save
some.”
DR. GEOFFREY CUNDIFF—
REGIONAL HEAD
OF OBSTETRICS AND GYNECOLOGY
SUNDAY, AUGUST 26, 2012A14 | SPECIAL SERIES | THEPROVINCE.COM
5. A12 MONDAY, AUGUST 27, 2012| THEPROVINCE.COM
beatheart
Inside St. Paul’s
Hospital
Spend a week in a maternity ward and you’ll see the
extraordinary lengths to which women will go to
bring new life into the world. Here, women brave pain
and illness, bedrest and diagnostic tests, surgery and
sleepless nights to birth their babies safely. And when
it’s hard, the staff of St. Paul’s are there. This week,
The Province tells the intimate stories of new families
created here and the care that makes it possible.
ELAINE O’CONNOR
THE PROVINCE
T
he day after giving birth to
her first child should have
been one of the best days of
LindsayEpp’slife.YetfortheLad-
ner mother “it was the worst day
of my life. It was horrible.”
Instead of cuddling her new-
bornbabygirl,AnnaMarieGrace
Epp, mother and baby were split
apart due to separate medical
emergencies.
Epp developed a life-threaten-
ing condition called HELLP syn-
dromeandwassenttotheinten-
sive-care unit at St. Paul’s, while
herdaughterstruggledtobreathe
andwastransferredtoB.C.Chil-
dren’s Hospital.
Epp had already been at St.
Paul’sonbedrestforweeksdueto
high blood pressure and a risk of
pre-eclampsia, a form of hyper-
tension. Her baby was delivered
prematurely by C-section at 34
weeks and was sent to the neo-
natal intensive-care unit.
But because her lungs were so
immature, she needed to go on
a ventilator, which required a
transfer to a higher-level NICU
at Children’s Hospital (a Level 3
NICU; St. Paul’s is Level 2).
That same day, her mother’s
systems started to fail. HELLP
syndrome involves a cascade of
symptoms:hemolysis(thebreak-
down of red blood cells), elevat-
ed liver enzymes and low blood
platelet count. The condition
occursinjustoneortwoofevery
thousand pregnancies. Women
often present with simple head-
aches, nausea and vomiting, but
theconditioncanleadtohemor-
rhaging and liver failure.
With the expertise of St. Paul’s
staff, Epp was stabilized and dis-
charged on Aug. 4, finally able
to travel to visit her daughter.
Her baby’s breathing improved
enough for her to come back to
St. Paul’s four days later.
OnlyEpp’shealthtrialsweren’t
over. On Aug. 10, she suffered
excessive postpartum bleeding
andhadtoundergoanemergen-
cy procedure.
“It’satoughone,”chiefmaterni-
tyresidentDr.MinaWesasaysof
theneedtoseparatesickmothers
from their infants. “A big part of
our discharge planning and the
goal of our patient care is mini-
mizing the separation between
mom and baby.”
Watching Epp calmly rock her
four-pound, five-ounce girl and
caress her wispy gold hair in
the NICU days later, it’s hard to
imagine the tribulations they
suffered to be together.
“She was worth every moment
ofhorribleness,”Eppsays,gazing
at her fragile daughter adoring-
ly. Having her safe, she says, “is
an incredible joy. There are no
words. I would do it all again in
a heartbeat for her.”
■
As frightening as Epp’s ordeal
sounds,treatingdesperatelysick
mothers like her is routine at St.
Paul’s.
“We take care of the high-risk
mothersintheprovince,”explains
maternity and NICU operations
leader Jackie Koufie.
There is certainly no shortage
of cases. In their daily morning
meeting, maternity doctors and
residents troubleshoot the preg-
nancies of women with multi-
ple complications, among them
patients with heart disease, dia-
betes, arthritis and pacemak-
ers. The residents speak in cryp-
tic code; acronyms fly. It sounds
every bit like the script of a med-
ical drama.
But these cases are very real
and in some cases these moth-
ers’conditionsarelifeanddeath
matters.
Todealwiththem,St.Paul’shas
establishedanumberofspecial-
ized clinics that bring specialist
care and additional oversight to
bear on their pregnancies.
Amongthemareinnovativecar-
diac obstetrics and renal obstet-
rics clinics, where patients are
referred from across the prov-
ince.
“It’s very frequent that patients
withheartdiseasehavebeentold
thattheycan’tbecomepregnant,”
sayscardiacobstetricclinicdirec-
B.C.’s haven
for sick moms
Lindsay Epp kisses daughter Anna in the neonatal intensive-care unit. Both mother and
baby had medical emergencies after Anna’s birth. JENELLE SCHNEIDER PHOTOS/PNG
Little Anna Epp’s wrists are as
thick as her mother’s fingers.
Heartbeat is an eight-month special series for which The Province has been granted
special access to St. Paul’s Hospital. The series runs for a week each month until November.
6. A13THEPROVINCE.COM |MONDAY, AUGUST 27, 2012
“I rarely get the simple consultations. Most patients who see me have three or four medical problems.”
— Dr. Duncan Farquharson
Dr. Marla Kiess listens to the heart of Sarah Bare, 27,
who is pregnant and suffers from tachycardia.
ELAINE O’CONNOR
THE PROVINCE
Sarah Bare’s heart is racing, and it’s
not because she’s nervous about her
first pregnancy.
The 27-year-old suffers from tachy-
cardia — an inefficient, rapid heart-
beat that reduces blood flow to the
body — which came on unexpected-
lyin2009duringabreathlessepisode
at work.
Luckily, the Squamish resident —
herself a trained cardiac care nurse
— was working in an Edmonton hos-
pital at the time. She knew enough to
gototheemergencydepartment,and
they found her heart racing at up to
180beatsperminute.Foranadult,100
is the upper threshold for normal.
Her condition was controlled with
medication,butBareworrieditwould
bar her from having a family.
“My doctor always said there might
beanissuegettingpregnant,”shesays,
sitting in an exam room in St. Paul’s
cardiac obstetric clinic with her hus-
band, Bryan, by her side.
So she was referred here, and her
baby,nowgrowingwelland21weeks
along, is being carefully monitored.
With this clinic, cardiologists Dr.
Marla Kiess and Dr. Jasmine Grewal
are helping mothers with heart con-
ditions who would once be warned
against pregnancy to fill their hearts
with joy.
“It’s kind of a unique area,” says
clinic director Dr. Kiess.
These days, women with heart dis-
ease, women who have had heart
attacksorcongenitalheartmalforma-
tions or even past transplant recipi-
entscangivebirthsafelywiththeright
kind of care — something unheard of
agenerationago,whensuchpregnan-
cies could be fatal.
“Ithinkthatwe’vereducedthemor-
tality rate since we started the clinic,”
Dr. Kiess says proudly. “We’ve defi-
nitely seen a significant reduction in
the number of complications.”
The cases they see are remarkably
complex. Some women have pulmo-
nary hypertension, a condition with
a mortality rate of up to 50 per cent.
Others will need valve replacement
surgery before pregnancy.
In rare cases, they have even per-
formedheartsurgeryonwomenwho
are pregnant, although the hospi-
tal stresses that this happens only in
extreme cases where circumstances
absolutely necessitate it.
The clinic runs three times a month
andhasbeengrowingquickly—they
have seen some 400 patients from
acrossB.C.overtheyears—butitruns
on a shoestring.
With more funding they’d like to
expand to help more women like
Bare, who, with luck and with extra
care from St. Paul’s, will get the gift of
a healthy baby boy this December.
Heart problems not the
barrier they once were
torDr.MarlaKiess,whofounded
the program in 2004. “And that’s
generally not the case.”
Obstetrician Dr. Elisabet Joa
established a similar clinic for
renalpatientsin2010withneph-
rologistDr.MonicaBruner,help-
ingaboutadozenwomendialy-
sispatientsandtransplantrecip-
ients achieve healthy pregnan-
cies each year.
Maternal fetal medicine con-
sultant Dr. Duncan Farquhar-
son monitors women with con-
ditionssuchasobesity,diabetes,
advanced maternal age, a histo-
ryofmiscarriage,geneticcondi-
tions and hypertension, as well
as those with heart and kidney
issues.
“Irarelygetthesimpleconsul-
tations. Most patients who see
me have three or four medical
problems,” says Dr. Farquhar-
son, who has spent 30 years
in obstetrics.
Many of the women he sees
arealiveduetoadvancesinfetal
medicine a generation ago.
“We see so many women now
who would not have been able
to achieve a pregnancy 20 years
ago,” he says. “Now some of
those fetuses I saw are becom-
ing moms, so full circle.”
As part of their care plan,
almostallthesehigh-riskmoth-
erswillvisitthefetalmonitoring
clinic, where nurses attach sen-
sors to their bellies and listen to
theirbabies’heartratestoensure
theyarefaringwelldespitetheir
mothers’ health issues. Patients
visit regularly, in the most seri-
ous cases even several times a
week,togiveclinicianstheassur-
ance they need.
“These ladies are the ones
who have pregnancy-induced
complications, for example,
gestational diabetes, gestation-
al hypertension, obese patients,
post-dates patients . . . it’s a very
busy clinic,” says nurse Roman
Djene.
Because of its high-risk
patients,thecliniccanbeahigh-
stakes environment.
Onewoman,Djenesaid,came
inforroutinefetalmonitoringat
34weeksonherlunchbreak.Her
strips were abnormal and she
needed a STAT C-section. So
much for returning to work.
■
Desiree Gano likely owes her
life to the specialized care at
St. Paul’s.
The 39-year-old mother had a
baby boy, Jonree Nathan Gano,
via C-section at 35 weeks ear-
lier this month, and she’s still
recovering. But she’s not in the
maternityward.She’sinthecar-
diaccareunit,onacarefulcock-
tailofmedicationthatiskeeping
her potentially life-threatening
condition — pulmonary hyper-
tension — in check.
She was diagnosed after com-
plaining of shortness of breath
in July. Her condition can be
fatal for pregnant women and
their babies, and Gano, who
had no history of heart disease,
is extremely lucky it was caught.
“I was shocked,” Gano said of
herdiagnosis,whichwillrequire
follow-up care. “My first preg-
nancy was normal, no prob-
lems.”
The nurse brings in her four-
pound, nine-ounce baby from
the NICU for his feeding and
Gano carefully holds a tiny bot-
tle to his lips, cradling him in
herarms,whicharestillcovered
in IVs.
“You’re a good boy, my baby”
she murmurs down at himas he
sucks. Then she turns him over
and gently pats his back until he
gives up an adorable burp.
Gano smiles.
“He’s cute.”
eoconnor@theprovince.com
twitter.com/elainereporting
onlinetheprovince.com/heartbeat
Photos videos your feedback
Desiree Gano’s son Jonree gets a cuddle from his mom, who
was diagnosed with pulmonary hypertension while pregnant.