Build Community/Public Health Partner Call Summary
•
1 like•192 views

Lessons and tips from the peer group call on November 3, 2016, with communities/public health departments on how to work effectively with hospitals to address social determinants of health in their communities.

Recommended
Recommended
More Related Content
What's hot
What's hot (17)
Viewers also liked
Viewers also liked (20)
Similar to Build Community/Public Health Partner Call Summary
Similar to Build Community/Public Health Partner Call Summary (20)
More from Courtney Bartlett
More from Courtney Bartlett (11)
Recently uploaded
Recently uploaded (20)
Build Community/Public Health Partner Call Summary
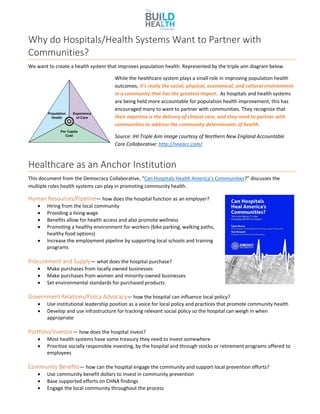
- 1. Why do Hospitals/Health Systems Want to Partner with Communities? We want to create a health system that improves population health. Represented by the triple aim diagram below. While the healthcare system plays a small role in improving population health outcomes, it’s really the social, physical, economical, and cultural environment in a community that has the greatest impact. As hospitals and health systems are being held more accountable for population health improvement, this has encouraged many to want to partner with communities. They recognize that their expertise is the delivery of clinical care, and they need to partner with communities to address the community determinants of health. Source: IHI Triple Aim image courtesy of Northern New England Accountable Care Collaborative: http://nneacc.com/ Healthcare as an Anchor Institution This document from the Democracy Collaborative, “Can Hospitals Health America’s Communities?” discusses the multiple roles health systems can play in promoting community health. Human Resources/Pipeline— how does the hospital function as an employer? Hiring from the local community Providing a living wage Benefits allow for health access and also promote wellness Promoting a healthy environment for workers (bike parking, walking paths, healthy food options) Increase the employment pipeline by supporting local schools and training programs Procurement and Supply— what does the hospital purchase? Make purchases from locally owned businesses Make purchases from women and minority-owned businesses Set environmental standards for purchased products Government Relations/Policy Advocacy— how the hospital can influence local policy? Use institutional leadership position as a voice for local policy and practices that promote community health Develop and use infrastructure for tracking relevant social policy so the hospital can weigh in when appropriate Portfolio/Investor— how does the hospital invest? Most health systems have some treasury they need to invest somewhere Prioritize socially responsible investing, by the hospital and through stocks or retirement programs offered to employees Community Benefits— how can the hospital engage the community and support local prevention efforts? Use community benefit dollars to invest in community prevention Base supported efforts on CHNA findings Engage the local community throughout the process
- 2. Tips for building relationships with hospital partners 1. Make sure the hospital partner knows the goals of the project up front Take time to orient them to their role in the project, the community served, and to the underlying causes of health inequity that you’re trying to address. 2. Match the goals of the project with the hospital priorities. Look at your hospital’s last Community Health Needs Assessment (CHNA) (these should be publically available and found online with a quick google search). Try to align the priorities identified in that assessment with your project goals. That will help garner support from the hospital since they will be able to see how the work can benefit them as well. More importantly, get engaged in the CHNA process the next time around! Try to get at the table for those conversations to begin building those relationships and influence the health equity discussion. EXAMPLE: One BUILD site’s partners were able to participate in the focus groups for the hospital’s CHNA process this year. Another BUILD site was part of their hospital’s first CHNA process a few years ago and has found that helpful to the current BUILD partnership in that it initiated some of that relationship building. EXAMPLE: In one BUILD city, community organizations and the health department were routinely approached by each of the hospitals in the area with the same series of questions and requests for population level data. Eventually, the health department convened all the hospitals who agreed to work on a joint CHNA with a core set of metrics that would serve the requirements. The hospitals decided to contract with the health department to produce the joint CHNA. They had great success in this process and are now entering the next phase to update it. Challenges to Collaborating on CHNAs/CHAs: Typically, health departments have to do a community health assessment (CHA) every five years, while hospitals complete their CHNA every three years. Thus it’s often difficult to sync the two calendars. The goal would be to have a joint assessment for the county that could be co-led by local health departments and health systems. 3. Identify the right person in the hospital system early on. EXAMPLE: One BUILD project began with a strong, accountable hospital partner, who had a thorough understanding of the project, understood the hospital’s role, and understood the social determinants of health in the project’s neighborhood. The hospital partner was planning to retire in the middle of the project, and in preparation for his departure, he appointed a colleague to step in early and ease the transition. They spent a lot of effort orienting this new person to the project to make sure she had the information needed to continue to support the hospital’s investment in the project. After 8 months of working with the new hospital partner, they learned there was actually a different person that oversees the hospitals community benefit funds, which were the source of the hospital’s investment in the project. They reinitiated efforts to update this other person on their efforts, but were pressed for time given the project deadlines. Ultimately, if they’d known to connect with the community benefits person from the beginning they could have saved a lot of time and effort. 4. Plan ahead, have a specific ask, and have exact numbers when possible If you know the exact amount of money (cash) needed from the hospital partner early on, that gives the hospital more time to plan and figure out how to allot the funds. It’s important that hospitals understand the direct link to health outcomes and their bottom line, and see how the work aligns with their mission.
- 3. EXAMPLE One BUILD site, due to staff transitions, didn’t know the exact cost of the project at the beginning of the planning period, and was only able to secure an in-kind match from the hospital, where cash would have been more beneficial to the project. If they had communicated the request earlier in the process, they might have secured more cash dollars in the match. 5. Keep the hospital engaged and informed on project deliverables and timelines throughout the project It’s important to keep the hospital partner engaged throughout the process, so they feel invested and you don’t just include them when it’s time to ask for funding support. Invite them to key meetings, and to be a part of the planning committees. 6. Find the best lane (fit) for the hospital system in the partnership It’s helpful to utilize the hospitals’ expertise and find the best fit for their skills in the structure of the partnership. They need to feel like they have the win from that relationship as much as the community does for having them at the table. EXAMPLE: The primary healthcare partner in one BUILD project is not a non-profit hospital, so they do not have the community benefit requirement. Therefore, their contribution to the work has been to provide evaluation support entirely in-kind, and significantly so, possibly even more than the 1:1 match requirement. The hospital has served as the lead evaluators for the project, including designing the shared measurement system, collecting data in the pre-test phase, and partnering with the local school of public health to analyze and publish the results. This has truly been a win-win for both the hospital and the community and a strength of the partnership, because they were able to identify that “best fit”. How Can Hospitals Support Communities? By providing funding support… Hospitals can use community benefit dollars to invest in community prevention. Many non-profit hospitals are this year in the process of completing their second CHNA as required by the IRS. SAMPLE BREAKDOWN OF HOSPITAL MATCH DOLLARS Funding salaries of two Community Health Workers $25,000 + in scholarships to high school students who will pursue careers in the healthcare industry $25,000 towards monitoring and evaluation – In-kind technical assistance $22,000 to train healthcare providers in target neighborhood BANDWIDTH – how much staff time does it take to drive the hospital/community partnership component forward? (e.g. effort and time commitment) ONE BUILD SITE FUNDS A 50% FTE PROJECT/NETWORK “WEAVER”. THEY ALSO HAVE AN IN-KIND PROJECT WEAVER FROM THE CITY, AND FROM THE HOSPITAL. THEY HAVE FOUND IT IMPORTANT TO HAVE A DEDICATED STAFF PERSON FROM EACH SYSTEM. GRADUATE FELLOWS FOCUSING ON POLICY WERE ALSO PLACED IN EACH OFFICE TO INCREASE STAFF CAPACITY. IF YOU DON’T HAVE THE RESOURCES, IT’S NOT A LOST CAUSE! WHAT YOU CAN’T DO IN VOLUME YOU CAN OFTEN DO OVER TIME.
- 4. SAMPLE BREAKDOWN OF HOSPITAL MATCH DOLLARS Funding cost for Community Health Workers to co-locate in health department office Share the rent for that office In another BUILD site, the hospital exceeded the 1:1 match and also invested $39,000 in a clinical community health worker pilot $5,000 in training for that team In addition to funding, hospitals can… 1. Heighten awareness and bring legitimacy to the work Having a major institution like the hospital at the table, often allows communities to capture the attention of mainstream audiences and key decision-makers. EXAMPLE: One BUILD site leveraged the relationship between their city planning and city community services departments, and the hospital. The city departments had great relationships with the hospital community benefits partner and having the hospital partner at the table brought legitimacy to their request to the city for support on their project. 2. Advocate in policy and systems change work EXAMPLE: One BUILD community developed a comprehensive budget request for the city council (nearly $60 million for staffing, operations, and capital investments to address public safety issues). The hospital provided support by adding their voice to the cause. The Hospital CEO wrote a letter to the city council supporting the budget request emphasizing that they as a hospital were happy to support this cause, but that it is ultimately the city government’s responsibility to address public safety in their neighborhoods. The CEO encouraged city council to at least match the hospital’s contribution to the BUILD project. The city council was impressed that a major institution (with an emphasis on healthcare) was stepping up to influence policy around public safety. How do you engage hospitals in upstream interventions? Many communities have found it challenging to translate their community action plans, which are centered on upstream interventions and do not involve a lot of clinical interventions, to something the hospital can get involved in. There is often a disconnect and finding the hospital’s significant role in implementing the community action plan can prove challenging. 1. Frame issues (e.g. housing, public safety, access to green space) in ways that align to a direct delivery of some kind of service. It’s important to translate the budget for the hospital/health system in terms of delivery of services. EXAMPLE: One BUILD site is creating a Housing and Healthcare partnership to facilitate sustainable relationships between hospitals and affordable housing providers to bring resources and education directly to residents in affordable housing buildings. The hospital feels comfortable providing those health education resources, so that was one way to plug them into the intervention. The community organization learned to find those places where hospitals feel comfortable providing services, but also recognize that they are not going to be the ones looking at economic development. It’s important to speak a language that appeals to them and ultimately to the hospital board that approves the funding. 2. Remember that Hospitals are Businesses A hospital’s reputation in a community helps them achieve market share in a competitive market, e.g. people want to go to their hospital because they believe that hospital is doing good in the community.
- 5. 3. Communities can help hospitals reduce their cost Hospitals are legally required to serve uninsured patients – that is a cost for the hospital. We can make the case that if community environments were better, that would reduce illness/injury rates and drive down costs for the uninsured. Hospitals would be able to then devote resources away from unnecessary illness/injury, and towards the more complex patients. Addressing Power Dynamics How do you work equitably with an organization that has much more power and resources than you do? We’re all trying to reduce disparities and improve health equity, but we first need to reduce inequity within our own partnerships. By design, community-based organizations are usually small, grassroots organizations. Because of the BUILD 1:1 dollar match requirement with hospitals, the burden falls on the community organization to appeal to these major institutions (hospitals) who carry a lot of financial power, political power, and general size. So naturally that leads to unequal power dynamics. How can we start the processes in a way to facilitate more equitable partnerships? 1. Coach hospitals to approach meetings with collaborative members differently than they are used to: Hospital partners need to come as listeners and learners. Hospitals are used to being in leadership roles, but need to rethink roles for equitable partnerships. - Speak last – if they speak first and take up all the oxygen in the room, the power dynamics are such that community members often won’t speak up after that. 2. Lead with metrics/framework previously defined and validated For initial planning meetings, lead with common metrics or goals (perhaps from Community Health Improvement Plan- something the hospital has already been involved in) to start the conversation about resource blending/braiding and strategy alignment. By doing so you can sometimes cut through the power dynamics. Data is powerful and having a clear vision about how these systems can work together can help the community org bring some power to the table. 3. Ask people to use reflective listening techniques Before you talk, reframe what someone just told you. This technique helps people: 1) know you were listening to them 2) know that you heard them correctly 4. Negotiation skills in general are helpful to address power dynamics. 5. Good facilitation can help equalize the power dynamics in the room For meetings, have a facilitator who is aware of some of these power dynamics. They can use facilitation techniques to address those issues during the meeting.