

Empfohlen
Weitere ähnliche Inhalte
Was ist angesagt?
Was ist angesagt? (20)
Ähnlich wie 4 u1.0-b978-1-4160-4224-2..50040-5..docpdf
Ähnlich wie 4 u1.0-b978-1-4160-4224-2..50040-5..docpdf (20)
Mehr von Loveis1able Khumpuangdee
Mehr von Loveis1able Khumpuangdee (20)
Kürzlich hochgeladen
Kürzlich hochgeladen (20)
4 u1.0-b978-1-4160-4224-2..50040-5..docpdf
- 1. Chapter 37 Placenta Previa, Placenta Accreta, Abruptio Placentae, and Vasa Previa Andrew D. Hull, MD, and Robert Resnik, MD Bleeding in the later stages of pregnancy has been described as “third- the cervix dilates or the lower uterine segment effaces. The term “low- trimester bleeding” or “antepartum hemorrhage.” Late pregnancy lying placenta” should be reserved for cases in which the placenta is bleeding is a significant cause of maternal and fetal morbidity, fetal seen on transabdominal ultrasound to extend into the lower uterine mortality, and preterm delivery. Traditional accounts of such bleeding segment but its precise limits have not been defined, and for cases have addressed placenta previa, abruptio placentae, and vasa previa, identified before the third trimester. TVUS allows location of the pla- although in fact the only thing that these clinical problems have in centa in relation to the internal cervical os with great precision. When common is that they all are concerned, to a greater or lesser extent, such studies are performed, the placenta may be classified as a complete with hemorrhage. The etiology, management, and complications of previa if it completely covers the internal os. The term marginal pla- each are quite distinct. In the past, uncertainty in precise diagnosis of centa previa should be used if the placental edge lies 2.5 cm or closer the cause of late pregnancy bleeding has led to these conditions being to the internal os. It has been shown that when the placenta is more considered together, but the universal availability of ultrasound tech- than 2 to 3 cm from the cervix, there is no increased risk of bleeding.2 nology has eliminated much of the diagnostic dilemma. A definitive diagnosis of placenta previa should be avoided in asymp- Bleeding during the second half of pregnancy complicates about tomatic patients before the third trimester, because many cases of pla- 6% of all pregnancies. Placenta previa is ultimately documented in 7% centa previa identified early in pregnancy will resolve as pregnancy of cases, and evidence of significant placental abruption is found in advances. 13%. In the remaining 80% of cases, the bleeding can be ascribed to Placenta previa affects about 1 (0.5%) of every 200 pregnancies at either early labor or local lesions of the lower genital tract or no source term.3 There is some evidence that the incidence of placenta previa is can be identified.1 Faced with a woman with late pregnancy bleeding, increasing.4 This increase may be related to the increasing rate of the clinician must rapidly reach a firm diagnosis and management plan cesarean section observed in all developed countries. A single prior to ensure the optimum outcome for mother and baby. Ultrasonogra- cesarean section or a prior pregnancy complicated by placenta previa phy, electronic fetal monitoring, and, frequently, evaluation of the increases the incidence of placenta previa in a subsequent pregnancy function of the maternal coagulation system make up the foundation to as high as 5%,1,5,6 rising even further with a history of more prior on which both diagnosis and management are developed. Clinical cesarean deliveries.7 Advanced maternal age increases the incidence of assessment must occur simultaneously with imaging and fetal placenta previa to 2% after 35 years of age and 5% after age 40.7 Mul- assessment. tiparity, prior suction curettage, and smoking are all associated with In asymptomatic patients who are without antenatal bleeding but higher risks of placenta previa.8-10 The relative risks for these associated have been identified by prenatal ultrasound as having risk factors (pla- factors are summarized in Table 37-1. centa previa, placenta accreta, or vasa previa), timing of delivery is the most important clinical decision that has to be made. Pathogenesis The underlying cause of placenta previa is unknown. There is a clear association between placental implantation in the lower uterine Placenta Previa segment and prior endometrial damage and uterine scarring from curettage, surgical insult, prior placenta previa, and multiple prior Definition and Epidemiology pregnancies. Advances in the precision of sonographic diagnosis, particularly trans- At least 90% of placentas identified as being “low lying” in early vaginal ultrasound (TVUS) technology, as well as an increased under- pregnancy will ultimately resolve by the third trimester.11 The term standing of the changing relationship between the placenta and the “placental migration” is widely used to describe this phenomenon. The internal cervical os as pregnancy advances, have rendered traditional placenta clearly does not move; rather, it is likely that the placenta definitions and classifications of placenta previa obsolete. Placenta grows toward the better blood supply at the fundus, a process known previa exists when the placenta covers the cervix either completely or as trophotropism, leaving the distal portions of the placenta, closer to partially or extends close enough to the cervix to cause bleeding when the relatively poor blood supply of the lower segment, to regress and
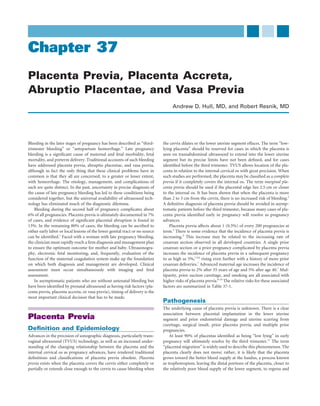
- 2. 726 CHAPTER 37 Placenta Previa, Placenta Accreta, Abruptio Placentae, and Vasa Previa atrophy. As the uterus grows and expands to accommodate the devel- onset of labor. Some women experience pain secondary to uterine oping fetus, there is differential growth of the lower segment, and this contractions. Bleeding may be provoked by labor, examination, or may further increase the distance between the lower edge of the pla- intercourse but it usually has no identifiable precipitating cause. The centa and the cervix. patient is more likely to have a fetus with an abnormal lie, inasmuch Bleeding from placenta previa may occur before labor as a result of as the placenta previa may prevent the fetus from establishing normal development of the lower uterine segment and effacement of the cervix polarity. All women presenting with painless vaginal bleeding after 20 with advancing gestation. Prelabor uterine contractions may also weeks’ gestation should be assumed to have a placenta previa until produce bleeding, as may intercourse or injudicious vaginal examina- proven otherwise. Transabdominal ultrasound should be quickly uti- tion. Once labor begins, significant bleeding will occur as the cervix lized to screen for placenta previa. Unless the placenta is clearly fundal dilates and the placenta is forced to separate from the underlying and the lower segment is clear, TVUS should then be performed. decidua. Transabdominal ultrasound has been shown to be inferior to TVUS for definitive placental localization.12,13 Concerns regarding the poten- tial for TVUS to provoke bleeding are unfounded, and several studies Diagnosis have confirmed the safety of a careful TVUS approach (Fig. 37-1).7,13,14 The classic history for placenta previa is that of painless third-trimester The placement of the transvaginal probe should be observed continu- bleeding. Several small “herald bleeds” may occur in advance of major ously on the ultrasound monitor during insertion, to avoid placing the hemorrhage, but in up to 10% of cases there is no bleeding until the probe into a potentially dilated cervix. If a transvaginal probe is unavailable, translabial imaging using a regular abdominal probe can produce excellent results, with better visualization of the relationship TABLE 37-1 RISK FACTORS AND RELATIVE between the cervix and placenta than is obtained from transabdominal scanning.15 A digital or speculum examination to inspect the cervix for RISKS OF PLACENTA PREVIA local causes of bleeding should not be performed until placenta previa Risk Factor Increased Risk Reference has been excluded by ultrasonography. In the unusual setting of significant late pregnancy bleeding where Previous placenta 83× Monica and Lilja, 1995 ultrasound is not available and the diagnosis is not clear, there is still previa a place for the “double-setup” examination. The patient is taken to the Previous cesarean 1.5-153× Herschkowitz et al, 1995; section Hemminki and operating room, where preparations are made for a cesarean delivery. Merilainen, 1996 A vaginal examination is then performed, beginning in the vaginal Previous suction 1.33× Taylor et al, 1994 fornices and avoiding placing the fingers directly in the cervix. If a curettage for placenta previa is detected, cesarean section is then performed. If no abortion placenta previa is found, a search for other causes of third-trimester Age > 35 yr 4.73× Iyasu et al, 1993 bleeding ensues. Age > 40 yr 93× Ananth et al, 1996 Multiparity 1.1-1.73× Williams and Mittendorf, Implications of Early Pregnancy Diagnosis 1993 The routine use of ultrasonography in the first and second trimesters Nonwhite race (all) 0.33× Iyasu et al, 1993 of pregnancy has led to the frequent observation of a low-lying pla- Asian race 1.93× Iyasu et al, 1993 Cigarette smoking 1.4-33× Handler et al, 1994; centa or a previa. Ananth, Savits, and Transabdominal ultrasound tends to over-diagnose low-lying pla- Luther, 1996; Chelmow centa, especially when the bladder is empty.16 Even with TVUS, the et al, 1996 findings may not correlate with the placental position at term. Several reports confirm that up to 10 times as many women are found to have B A FIGURE 37-1 Ultrasound study performed at 18 weeks’ gestation for fetal anatomy survey. A, Transabdominal ultrasound shows an apparent “low-lying placenta.” B, Transvaginal ultrasound shows that the placenta completely covers the cervix.
- 3. CHAPTER 37 Placenta Previa, Placenta Accreta, Abruptio Placentae, and Vasa Previa 727 a placenta previa in the second or first trimester than at delivery.14,17-21 the less likely it is that a significant prolongation of pregnancy will be The earlier in pregnancy a diagnosis of placenta previa is made, the gained.26 Betamethasone to enhance fetal lung maturation should be less likely it is that the finding will persist at delivery.22 The likelihood administered to patients who are at less than 34 weeks’ gestation if of persistence to term of a placenta previa found in the second trimes- expectant management is planned. ter is also related to the degree to which the placenta overlies the There is controversy regarding the role of tocolytics in the setting cervix14,17-21 and the thickness of the placental edge.23 It is recom- of hemorrhage from placenta previa. Both β-mimetics and magnesium mended that a follow-up ultrasound study be performed between 28 sulfate27-29 have been used in this setting and appear to be associated and 32 weeks’ gestation to further evaluate the placental position. If with significant prolongation of pregnancy without adverse effects. there appears to be a significant change in the position of the placental After the initial presentation with bleeding, patients should remain edge over time, a final study should be done at 36 weeks, before making in hospital until they are free of bleeding for at least 48 hours. Some a final decision as to the appropriate route of delivery. may then be considered for home management. Several studies have addressed the issue of safety of outpatient management in a controlled setting at home.25,30-33 With the exception of one report of an increase Management in perinatal mortality and morbidity and earlier gestational age,34 it Any woman with vaginal bleeding after 20 weeks’ gestation should be appears to be a safe approach. Patients selected for home management assessed on a labor and delivery unit. The primary focus should be on should be asymptomatic with regard to bleeding and abdominal pain, hemodynamic assessment of the mother and assessment of fetal well- be able to remain at home with limited activity, and have adequate being. Vital signs are obtained, and electronic fetal monitoring initi- support as well as adequate access to transport to a nearby hospital if ated. One or two large-gauge intravenous lines should be placed, and bleeding recurs. A second significant bleeding episode usually results maternal blood should be sent for determination of the hematocrit in readmission until delivery. and type and screen. For substantial bleeding episodes, 2 to 4 units of Several strategies have been proposed to reduce the risk of hemor- blood should be cross-matched. Obstetric units might consider the use rhage in women with a known placenta previa. Bed rest, reduced of an “Obstetric Hemorrhage Protocol” to facilitate access to the activity, and avoidance of intercourse are commonly mandated and resources of the hospital blood bank for this and any other obstetric seem logical, although there is no conclusive evidence to support these hemorrhage (Table 37-2). Rh immune globulin is administered, when measures. Cervical cerclage was evaluated in two small prospective appropriate, to Rh-negative, nonimmunized women. studies35,36 without clear benefit and is not recommended. Once the patient is stabilized and fetal condition has been assessed, All women whose placenta lies within 2 cm of the cervix, as docu- the definitive cause of the bleeding can be addressed. If the diagnosis mented by a late third-trimester TVUS scan, should be delivered by is clearly placenta previa and the patient is at or beyond 36 weeks’ cesarean section.37-39 An asymptomatic woman whose placenta lies gestation, delivery is appropriate. If bleeding is excessive or continues, more than 2 cm from the cervical os can be allowed to labor safely.16 or if there are concerns about the condition of the fetus, the patient It should be noted that the presence of a low-lying placenta, even if it should be delivered regardless of gestational age. In all other cases, does not cause intrapartum bleeding, increases the risk of postpartum management may be conservative and has been shown to be safe,24,25 hemorrhage because of lower uterine segment atony. with prolongation of pregnancy by an average of 4 weeks after the Cesarean section for placenta previa should be performed by the initial bleeding episode. The closer it is to a gestational age of 36 weeks, most experienced team available because of the substantial risk of intraoperative hemorrhage.40 In most instances, a lower uterine segment incision is appropriate. If the placenta is anterior, it is neces- sary to clamp the umbilical cord immediately to prevent excessive TABLE 37-2 OBSTETRIC HEMORRHAGE blood loss caused by disruption of the placenta during entry. A vertical PROTOCOL incision is also reasonable in such cases and may be preferable if the Blood is immediately drawn and set up for fetus is premature or if a transverse lie exists.41 Postpartum hemor- Type and cross-matching rhage may occur from the placental implantation site secondary to Hematocrit atony and may require the use of additional pharmacologic agents to Coagulation studies (PT/PTT/fibrinogen) control blood loss, such as methylergonovine maleate (Methergine), Wall clot (blood is drawn into a plain tube and set aside—should 15-methyl prostaglandin F2α (Hemabate), and high-dose oxytocin, clot within 6 min) used either singly or in combination. The B-Lynch suture42 or local An ABG determination may be requested to assess acute blood suturing of the placental bed may be needed to control bleeding. In loss (typically, every increment in base deficit of −1 to −2 rare cases of refractory hemorrhage, hysterectomy may be required. requires 1 unit of PRBCs to correct it) Among women known to have a placenta previa who do not require Four units of type-specific or O-negative blood are made very early delivery, elective delivery should be performed before sig- immediately available. The laboratory immediately starts to cross-match 4 units of blood nificant bleeding has occurred. It is reasonable to plan on delivery at and stays 4 units ahead of blood use. or just after 36 weeks’ gestation, because there is little fetal advantage Two units of FFP are thawed and made available. after that time, when weighed against the risk of a sudden and possibly One 10-pack of platelets is made available. excessive bleeding episode. The alternative is to perform an amniocen- The blood bank is alerted to provide further units of blood, FFP, tesis to confirm lung maturity before delivery, but the risk of hemor- and platelets as needed. rhage with delayed delivery usually outweighs the risk of fetal lung Further samples for ABGs and other laboratory studies are drawn immaturity at that gestational age. as required. The selection of anesthesia to be used for cesarean section in cases ABGs, arterial blood gases; FFP, fresh-frozen plasma; PRBCs, packed of placenta previa should be decided by the obstetrician and anesthe- red blood cells; PT, prothrombin time; PTT, partial thromboplastin siologist involved with the delivery, in concert with the patient. In the time. United Kingdom, regional anesthesia was preferred by most obstetric
- 4. 728 CHAPTER 37 Placenta Previa, Placenta Accreta, Abruptio Placentae, and Vasa Previa anesthesiologists in a survey43 and was used in 60% of cases in a ret- with placenta previa and prior uterine surgery.46,47 In patients with rospective series.44 Regional anesthesia is associated with lower opera- placenta previa, the risk of accreta is 10% to 25% with one prior cesar- tive blood loss and less need for transfusion than general anesthesia,3,45 ean section and exceeds 50% with two or more prior cesareans.48-50 probably because many inhaled anesthetics cause uterine relaxation. Prevalence appears to be similar in women with these risk factors undergoing second-trimester pregnancy termination.51 The diagnosis of placental invasion of the myometrium usually can Complications be made by ultrasound,52-54 with a reported sensitivity and specificity for the diagnosis of approximately 0.8 and 0.95, respectively.53,55,56 Mag- Placenta Accreta netic resonance imaging (MRI) has also been used to confirm the One of the most serious complications of placenta previa is the devel- diagnosis or better delineate the presence or extent of accreta.53 MRI opment of placenta accreta. This condition involves trophoblastic inva- is also useful in the presence of a posterior placenta and in the assess- sion beyond the normal boundary established by the Nitabuch fibrinoid ment of deep myometrial, parametrial, and bladder involvement.55,57 layer. If invasion extends into the myometrium, the term placenta The ultrasound appearance of a normal placental attachment site increta is used; placental invasion beyond the uterine serosa (at times is shown in Figure 37-3A. Normal attachment is characterized by a involving the bladder or other pelvic organs and vessels) is termed homogeneous appearance of the placenta and a hypoechoic boundary placenta percreta. Histologic examples of normal placental implanta- tion and placenta accreta are shown in Figure 37-2. Placenta accreta is associated positively with advanced maternal age, smoking, and parity, but the strongest recognized association is B P C P A B P C B FIGURE 37-3 Ultrasound appearance of a normal placental attachment site and placenta accreta. A, Normal placental attachment in an anterior placenta previa. A hypoechoic area FIGURE 37-2 Histologic appearance of normal placental separates the bladder wall and the placental tissue, representing implantation and placenta accreta. A, Histologic section of a myometrium and myometrial vasculature. B, Characteristic ultrasound normal placental attachment site. Trophoblastic tissue with anchoring appearance of placenta accreta. Note the lack of a hypoechoic area, villi encroach but do not go through the Nitabuch membrane. as well as obliteration of the well-delineated bladder wall. In addition, B, Representative histologic section of placenta accreta, there are intraplacental sonolucent spaces (arrows) adjacent to the demonstrating invasion of trophoblasts into the myometrial tissue. involved uterine wall. B, bladder; C, cervix; P, placenta.
- 5. CHAPTER 37 Placenta Previa, Placenta Accreta, Abruptio Placentae, and Vasa Previa 729 between the placenta and the bladder that represents the myometrium and the normal retroplacental myometrial vasculature. The bladder wall is intact throughout. In contrast, placental accreta is associated Vasa Previa with loss of the normal hypoechoic boundary, and there are usually intraplacental sonolucent spaces adjacent to the involved uterine wall Definition and Epidemiology (see Fig. 37-3B). Color-flow and power Doppler sonography have also Vasa previa is a rare but potentially catastrophic complication in which been reported to facilitate the diagnosis.58-60 Chou and associates60 fetal vessels run through the fetal membranes and are at risk of rupture evaluated 80 women with placenta previa to determine the accuracy with consequent fetal exsanguination. It is estimated that vasa previa of color-flow Doppler ultrasonography in distinguishing between affects between 1 in 1275 and 1 in 8333 pregnancies.73,74 uncomplicated placenta previa and placenta accreta. Using their crite- ria, the antepartum diagnosis of accreta was made in 16 of the 80 women studied and was confirmed histopathologically in 14. The sen- Pathogenesis sitivity and specificity for diagnosis were 0.82 and 0.97, respectively. Vasa previa may occur because the insertion of the umbilical cord into Although it is clear that larger numbers of patients must be studied by the placenta is velamentous, with the umbilical vessels coursing through these various modalities to more accurately determine the sensitivities the fetal membranes before inserting into the placental disk and the and specificities of diagnosis, various types of ultrasonography and unsupported vessels then overlying the cervix. It may also result from MRI appear to hold promise in making or excluding the diagnosis in the presence of a bilobed or succenturiate placenta with the vessels most cases. connecting the placenta similarly overlying the cervix.16 If the condi- It is important, if at all possible, to make the diagnosis before deliv- tion goes unrecognized, it is associated with a fetal mortality rate of ery, because intraoperative hemorrhage can be massive, and placenta almost 60%. In addition to a succenturiate placenta75 and velamentous accreta has been reported to be the most common indication for emer- insertion, other risk factors include a low-lying placenta observed in gency peripartum hysterectomy.61,62 In an effort to diminish blood loss, the second trimester,76 multiple gestation, and in vitro fertilization.77 it is recommended that delivery be accomplished through a fundal incision followed by clamping of the cord. The placenta is allowed to remain in situ while the surgeons proceed to a total abdominal hyster- Diagnosis ectomy. This may require very complex surgical technique and plan- The key to reducing fetal loss from vasa previa is prenatal diagnosis.16 ning, and a pelvic surgeon capable of wide resection of the lower Many cases of vasa previa are identified only at the time of vessel uterine segment and parametrial areas should be available, as well as rupture in labor. Vaginal bleeding is followed by fetal distress and death ample transfusion capability. if emergent delivery cannot be effected in time. Because the entire fetal Although published reports are not extensive, it has been suggested cardiac output passes through the cord, it can take less than 10 minutes that balloon occlusion of the aorta or internal iliac vessels may help to for total exsanguination to occur. Electronic fetal monitoring may prevent excessive blood loss during resection of the lower uterine show an initial tachycardia, rapidly followed by decelerations, brady- segment. This involves preoperative placement of balloon-tipped cath- cardia, and a preterminal sinusoidal rhythm.78 If a cesarean delivery eters retrograde through the femoral arteries immediately before can be accomplished immediately and with sufficient rapidity, good surgery. The catheters are guided under fluoroscopic direction into the newborn outcome can be obtained by aggressive postnatal transfusion internal iliac arteries and inflated during the dissection. However, the therapy.79 value and safety of this approach have been challenged with the recent It has been suggested that the blood from the vagina may be tested reports of no proven benefit and embolic complications.63,64 Neverthe- to confirm its fetal origin, using the Apt or Kleihauer-Betke tests or less, the placement of catheters does provide the opportunity to manage electrophoresis.80 In actual practice, such tests are either unavailable or potential postoperative bleeding with angiographic embolization cannot be done quickly enough to be of any value. Occasionally, fetal rather than reexploration. vessels have reportedly been felt through the membranes during Conservative management may be an option if there is suspicion vaginal examination or visualized on amnioscopy; such observations of a small focal accreta, if there is a fundal location after a myomectomy are really only of historical interest in modern practice. or classic cesarean section, or with a posteriorly implanted placenta. A It is now well established that vasa previa may be diagnosed prena- few reports have suggested leaving the uterus and placenta in situ and tally using ultrasound.81,82 Routine obstetric ultrasound should include using methotrexate postoperatively.65-67 However, the numbers of an assessment of the placental site and number of placental lobes and reported cases are very few, and hemorrhagic and infectious complica- an evaluation of the placental cord insertion site. In all cases in which tions have usually resulted. Consequently, a definitive surgical approach a multilobed or succenturiate placenta or a low-lying placenta or vela- to this serious obstetric complication is strongly recommended. mentous cord insertion is identified using transabdominal ultrasound, a detailed examination of the lower uterine segment and cervix should Neonatal Complications be performed using TVUS. Gray-scale ultrasound can identify placen- It has been suggested that repetitive bleeding from placenta previa is tal cord insertion in most cases, but color or power Doppler makes the associated with fetal growth impairment,68 although this has been dis- process easier and should be used (Figs. 37-4 and 37-5).81-84 There have puted.26 Pregnancies complicated by placenta previa have also been been several studies evaluating this approach for prenatal detection of reported to be associated with higher rates of fetal anomalies,69 neuro- vasa previa,81,82,84,85 all of which showed high specificity and sensitivity developmental delay,70 and sudden infant death syndrome (SIDS).71 of detection with little impact on the length of scan time. More impor- The reasons for these findings are unknown. tantly, in cases in which vasa previa was detected prenatally, there were As might be expected, placenta previa and previa accreta are a cause no fetal deaths from the condition. A recent retrospective, multicenter of preterm birth due to the need for iatrogenic preterm delivery. study showed newborn survival rates of 97% in prenatally detected Accreta has also been reported to have a negative influence on fetal cases of vasa previa and a fetal loss rate of 56% in cases not identified growth (odds ratio, 5.05 compared with controls).72 before the commencement of labor.86 Newer imaging modalities such
- 6. 730 CHAPTER 37 Placenta Previa, Placenta Accreta, Abruptio Placentae, and Vasa Previa B A D C FIGURE 37-4 Vasa previa identified at 18 weeks’ gestation on routine ultrasound studies. A, Transabdominal power Doppler identifies the umbilical cord possibly overlying the cervix. B, A fetal arterial waveform using power and pulse-wave Doppler. C, Vasa previa in gray scale on transvaginal ultrasound. D, Confirmation of the vasa previa using color Doppler transvaginally. because the vessels may be compressed by the presenting part and thus difficult to visualize. Management There is no uniformity of opinion as to the optimal management strategy for pregnancies with a prenatally diagnosed vasa previa, par- ticularly in regard to the timing of elective delivery. It has been sug- gested that patients be hospitalized at 30 to 32 weeks and delivered at 35 to 36 weeks’ gestation without confirmation of lung maturity by amniocentesis.16 This approach is based on the 10% risk of membrane rupture before labor and the high associated fetal mortality rate. Our approach has been to assess cervical length weekly from at least 30 weeks using TVUS. If the cervix is 2.5 cm in length or greater, out-of- FIGURE 37-5 Vasa previa. The placenta from the case identified in hospital management continues. The patient is administered beta- Figure 37-4. The patient was delivered by elective cesarean section at methasone just before 34 weeks’ gestation and is delivered by cesarean 34 weeks. Arrow shows velamentous cord insertion. section between 34 and 35 weeks, without additional testing for fetal lung maturity. as MRI87 and three-dimensional ultrasound have been described in the evaluation of vasa previa.87-89 MRI is of little practical use in routine Prevention of Adverse Outcomes cases. Although transvaginal three-dimensional power Doppler pro- A significant reduction in fetal mortality should be possible with a vides an excellent means of visualizing the entire lower uterine segment diligent search as previously described. Public and professional aware- for the evaluation of vasa previa, similar information may be obtained ness has been heightened by such organizations as The International by careful use of a two-dimensional vaginal probe. Such imaging com- Vasa Previa Foundation (http://www.vasaprevia.com [accessed Febru- bined with maternal positional change, the use of the Trendelenburg ary 8, 2008]). However, a high index of suspicion by the attending position, and gentle manual elevation of the fetal presenting part aid physician and a meticulous approach to diagnosis provide the best in visualizing the fetal vessels. The latter technique is particularly useful opportunity for a favorable outcome.
- 7. CHAPTER 37 Placenta Previa, Placenta Accreta, Abruptio Placentae, and Vasa Previa 731 of fetal nutrition. The process may be self-limited or ongoing with further dissection of the decidua. Dissection can lead to external bleed- Abruptio Placentae ing if it reaches the placental edge and tracks down between the fetal membranes; circumferential dissection leading to near-total separation Definition and Epidemiology of the placenta can occur, particularly with concealed abruption. The Abruptio placentae is the premature separation of a normally sited underlying event in many cases of abruption is thought to be vaso- placenta before birth, after 20 weeks’ gestation. It is a particularly haz- spasm of abnormal maternal arterioles. Some cases may result from ardous condition associated with significant maternal and fetal mor- venous hemorrhage into areas of the decidua that have become necrotic bidity and mortality. About 1% of all pregnancies are complicated by secondary to thrombosis. Long-standing predisposition to abruption clinically recognized abruption.90-93 The degree of abruption ranges may be inferred from the finding that women destined to suffer abrup- across a broad clinical spectrum, from minor degrees of placental tion have low levels of pregnancy-associated plasma protein A (PAPP- separation, with little effect on maternal or fetal outcome, to major A).105 Evidence of preexisting placental pathology in women with abruption associated with fetal death and maternal morbidity. Abrup- abruption includes poor trophoblastic invasion,106 inadequate remod- tion sufficient to cause fetal death occurs in about 1 of every 420 eling of the uterine circulation as reflected by abnormal uterine artery deliveries.94 If placentas are routinely examined after delivery, evidence Doppler flow,107 and the well-established associations among pre- of abruption may be found in almost 4% of cases, most of which were eclampsia, IUGR, and abruption—all of which may be regarded as unrecognized and of no apparent clinical consequence. There has been primary placental disorders. Abruption may also occur secondary to an increase of almost 25% in the rate of clinically detected abruption acute shearing forces affecting the placenta-decidua interface, such as in the United States in recent decades, with a disproportionate increase those that occur with trauma—particularly rapid deceleration injuries seen among African-American women.95 (motor vehicle accidents) and the sudden decompression of an over- The incidence of abruption peaks between 24 and 26 weeks’ gesta- distended uterus that occurs with membrane rupture in polyhydram- tion.96 Approximately 10% of all preterm births occur because of nios or delivery of a multiple gestation. abruption,90 and the infant outcomes are associated with increased As the abruption process continues, loss of placental function rates of perinatal asphyxia,97 intraventricular hemorrhage, periven- results in fetal hypoxia and may end in fetal death. The acute hemor- tricular leukomalacia,98 and cerebral palsy99 when compared with ges- rhage activates the coagulation cascade, and, with ongoing bleeding, tational age–matched controls. Perinatal mortality in pregnancies disseminated intravascular coagulation (DIC) may result. Continued complicated by abruption may be declining overall,93,100 but the rate bleeding, with maternal hypovolemia and poor tissue perfusion, aggra- continues to be higher than in gestational age–matched controls vates the DIC and results in a downward spiral into hemorrhagic without abruption.96 Placental separation is strongly associated with shock. Bleeding into the myometrial tissue can lead to a Couvelaire preterm premature rupture of the membranes (pPROM), in both a uterus which becomes atonic and increases the risk of uterine hemor- causal and a consequential manner.101 Most pregnancies complicated rhage after delivery. by abruption result in the delivery of an infant weighing less than the 10th percentile for gestational age,102-104 suggesting a common pathway Risk Factors and Associations for Abruption linking abruption to placental dysfunction and intrauterine growth The most important risk factor for abruption is a history of abruption retardation (IUGR). in a prior pregnancy.108 One meta-analysis showed an increase of up to 20-fold in the risk of abruption if a prior pregnancy had been simi- larly affected.109 With two prior pregnancies complicated by abruption, Pathogenesis the risk of recurrence is 25%.94 Abruption results from bleeding between the decidua and placenta Maternal hypertension is also a significant risk factor for abruption. (Fig. 37-6). The hemorrhage dissects the decidua apart, with loss of Chronic hypertension is associated with a fivefold increase in risk, the corresponding placental area for gaseous exchange and provision which rises to eightfold with superimposed preeclampsia.96 Preeclamp- sia alone is also strongly linked to abruption and to the severity of abruption.110 It seems plausible that preeclampsia and abruption share many underlying pathologic mechanisms. Perhaps the most readily preventable risk factor for abruption is cigarette smoking. Cigarette smokers are up to 2.5 times more likely to have an abruption than nonsmokers,111-115 and they have twice the perinatal mortality of nonsmokers.116 There is a dose-response rela- tionship between the number of cigarettes smoked and the risk of abruption.115,117,118 Even women who stop smoking before pregnancy are at increased risk. Substance abuse is closely linked to abruption— any agent that causes vasospasm or transient severe hypertension may be causative.119,120 In the United States, as many as 10% of pregnant women who are cocaine and crack cocaine users will experience pla- cental abruption.121 Multiparity is also positively correlated with a small increase in the risk of abruption.1,102 The apparent association between maternal age and abruption is not significant when parity is taken into account. There has been substantial recent interest in the possible association FIGURE 37-6 Abruptio placentae. A large retroplacental abruption between thrombophilic disorders and abruption. Some retrospective at 30 weeks’ gestation is shown. studies of abruption have found increased rates of thrombophilia.122,123
- 8. 732 CHAPTER 37 Placenta Previa, Placenta Accreta, Abruptio Placentae, and Vasa Previa However, both retrospective124 and prospective case-control studies125 hemorrhage. Fetal compromise is a common finding, and if more than of women with the factor V Leiden mutation showed no increase in 50% of the placenta is involved, fetal death is likely. Massive concealed abruption risk. It is established that hyperhomocysteinemia is associ- abruption often manifests with severe pain, a hard uterus, and a dead ated with abruption,123 although, in the absence of hyperhomocystein- fetus; such a picture may occur in association with severe preeclampsia emia, the specific MTHFR gene mutations themselves do not appear or the recent use of a vasoactive drug such as cocaine.139 If abruption to be associated with an increased risk.126,127 occurs in a posteriorly located placenta, severe back pain may be the Motor vehicle accidents are the most common traumatic event only symptom; it may be worsened by abdominal palpation that pushes associated with abruption, and clinical evidence of abruption may not the fetus against the placenta. Abruption may precipitate preterm be apparent for 24 hours or longer after the trauma. Women with labor, and it should always be considered in the differential diagnosis vaginal bleeding or contractions after a motor vehicle accident should for a patient in apparent idiopathic preterm labor. be observed for at least 24 hours; those who are asymptomatic can Although ultrasonography is an integral part of the diagnostic safely be discharged after 6 hours of monitoring.128,129 approach to late pregnancy bleeding, its utility is primarily for the Membrane rupture may precede or follow chronic retroplacental exclusion of placenta previa as the cause of hemorrhage. At least 50% bleeding or an acute abruption, and women with ruptured membranes of abruptions produce no findings on ultrasound.140-142 What is visual- should be monitored carefully for this possibility.109,130 Those with ized by ultrasound depends on the site, scale, and timing of bleeding. early pregnancy bleeding who have a subchorionic hematoma visible In early acute abruptions, blood and clot retained within the uterus on ultrasound are also at increased risk for both pPROM and appear as hyperechoic or isoechoic collections relative to placental abruption.131 echogenicity.143 In cases that remain undelivered, the hematomas Screening tests performed for other indications may identify groups resolve over several weeks, becoming hypoechoic and then sonolucent, of women who are at increased risk for abruption but may have no usually by 2 weeks after the event.143 Intrauterine clot may “jiggle” other high-risk factors. These tests include maternal first- and second- when bounced by the transducer—the “jello” sign. An acute abruption trimester serum screening for aneuploidy. Women with PAPP-A levels with obvious vaginal bleeding, in which little or no blood is retained below the 5th percentile at the time of first-trimester serum screening within the uterus, may have no specific sonographic findings. There- for trisomy 21 have an increased risk of abruption,105 but low levels of fore, the absence of ultrasound findings never excludes an abruption. human chorionic gonadotropin (hCG) in the first trimester are not Cardiotocography is an integral part of the evaluation for late preg- similarly associated.132 In one study of routine uterine artery Doppler nancy bleeding. Abruption is commonly accompanied by uterine con- velocimetry performed at 11 to 14 weeks’ gestation as a screen for tractions that may not be appreciated clinically, particularly after IUGR and preeclampsia, a pulsatility index higher than the 95th per- trauma.144 Fetal heart rate tracings may exhibit a variety of abnormal centile or a PAPP-A value lower than the 10th percentile predicted 43% patterns, including variable and late decelerations, poor variability, of pregnancies with a subsequent abruption.133 In an earlier study of prolonged bradycardia, or a sinusoidal pattern; these are not specific uterine artery Doppler ultrasound, persistent notching of the wave- to abruption and reflect underlying evolving fetal asphyxia. form after 24 weeks was associated with increased risk for abruption Kleihauer-Betke testing is of no diagnostic value in abruption: It as well as IUGR and preeclampsia.107 may be negative with proven abruption128,129,145 or positive when no Women with otherwise unexplained elevated serum levels (>2 mul- abruption has occurred. Its only value in this setting is to guide Rh tiples of the median [MOM]) of α-fetoprotein (AFP) on second-tri- immune globulin dosing in Rh-negative women who are thought to mester serum screening for trisomy 21 have long been thought to be have sustained an abruption. at increased risk for a wide range of adverse pregnancy outcomes, Chronic abruption-oligohydramnios sequence (CAOS) is a term including abruption.134,135 However, a recent case-matched, prospective that was coined to describe women who present with bleeding attrib- study found elevated AFP levels to be associated with an increased risk uted to abruption and go on to develop oligohydramnios without of abruption but no increase in the frequency of IUGR, preterm deliv- evidence of ruptured membranes.146 Twenty-four patients were ery, low birth weight, or fetal death.136 A recent attempt to establish a described, all of whom delivered preterm (average gestational age, 28 critical cutoff value for elevated AFP and increased risk of abruption weeks). For the most part, the earlier the onset of bleeding, the earlier stressed the low specificity and high false-positive rate of the test.136 the delivery. More than half of the women went on to develop pPROM Elevated hCG values at the time of second-trimester serum screen- before delivery and after the development of oligohydramnios. ing have similarly been associated with adverse pregnancy outcome, including abruption.137 Previously, a value greater than 2.0 MOM was thought to be significant in this context, but one recent case-controlled Management study showed that the threshold should be set at 3.0 MOM. Even at The key to optimizing maternal and fetal outcome in abruptio placen- that level, a positive test had poor predictive value and was not associ- tae is the individualization of care. Precise management depends on ated with increased risk of abruption.138 Abnormal inhibin values do the extent of maternal and/or fetal compromise and the gestational not appear to be predictive of abruption. age. Decision making should be rapid but methodical; delay in diag- nosis and inappropriate triage leads to significantly increased perinatal mortality.147 Twenty percent of all fetal deaths from abruption occur Diagnosis after presentation to the hospital, and 30% of those deaths occur The diagnosis of placental abruption is made based on clinical find- within 2 hours after admission. ings. The classic presentation is that of vaginal bleeding, usually Initial assessment should focus on maternal hemodynamic status accompanied by abdominal (uterine) pain. Examination often reveals (remembering that blood pressure may be elevated in the setting of uterine tenderness, and contractions may be present. About 10% of preeclampsia) and fetal well-being. Maternal vital signs should be mea- abruptions are concealed, with no vaginal bleeding. If bleeding is sured frequently, because they may change suddenly as the abruption present, the amount is often a poor guide to the degree of separation, evolves. Electronic fetal monitoring should begin immediately and be because there is usually a mixed picture of apparent and concealed continuous throughout further assessment and management. A large-
- 9. CHAPTER 37 Placenta Previa, Placenta Accreta, Abruptio Placentae, and Vasa Previa 733 gauge intravenous line should be placed (two lines if the patient is If the patient has sustained a mild separation at a premature gesta- hemodynamically unstable). Initial laboratory studies should include tional age and is asymptomatic without evidence of bleeding, discharge a baseline complete blood count and platelet count, type and screen home may be considered as an alternative to prolonged hospitalization. and cross-match where appropriate, blood urea nitrogen and electro- Either way, a clear management plan for delivery should be developed lytes, coagulation studies, and a wall clot. These studies serve as useful based on subsequent events or the reaching of an arbitrary gestational baseline references. An indwelling bladder catheter should be placed to age (usually 37 weeks). The evaluation of patients undergoing expect- allow urinary output to be closely monitored. In unstable or critically ant management should include regular assessment of fetal growth ill patients, management may be aided by placement of a central and tests of well-being, because these fetuses are at increased risk for venous pressure line (preferably with a Cordis introducer) or an arte- IUGR. rial line. The involvement of the obstetric anesthetic team should be If an abruption occurs after 34 weeks’ gestation and maternal sought early. and fetal condition permit, vaginal delivery is preferred. Amniotomy After these steps are taken, attention should be directed at excluding should be performed, and, if needed, an oxytocin infusion should a placenta previa (by ultrasound examination) and deciding on the be started. Labor usually progresses rapidly, even without augmenta- timing and route of delivery. Maternal or fetal compromise mandates tion. However, if progress is slow or maternal or fetal status deterio- immediate delivery, usually by cesarean section unless the patient is in rates, cesarean section should be performed. If abruption has resulted an advanced stage of labor. If the event occurs after 34 weeks’ gestation, in fetal death, vaginal delivery is preferred unless there are other delivery should not be delayed, because the risks of conservative man- obstetric contraindications or the mother is hemodynamically agement outweigh any considerations of prematurity of the fetus. unstable. Between 20 and 34 weeks, if mother and fetus are stable, an attempt at Coagulopathy develops in about 10% of abruptions. It usually is conservative management may be considered.148,149 Betamethasone related to the severity of the event and is particularly likely to occur if should be administered to enhance fetal lung maturity in all such cases. there is fetal demise or massive hemorrhage. An aggressive approach The patient should be monitored closely, because she continues to be should be used to maintain maternal blood volume and oxygen- at risk of an evolving process. The use of tocolytics is controversial; in carrying capacity, including the use of component therapy (fresh- most cases, they should not be used. Although studies addressing this frozen plasma and platelets). The coagulation tests most frequently issue have found no increase in adverse fetal or maternal events,27,141,148-150 used, and the component replacement therapy for women with DIC, no prospective trial has been performed. are summarized in Tables 37-3 and 37-4. TABLE 37-3 COAGULATION TESTS USED IN THE DIAGNOSIS OF ABRUPTIO PLACENTAE Test What It Measures Normal Value Value in Abruption Bleeding time Vascular integrity and platelet 1-5 min Usually normal; test is of little clinical use in function diagnosing abruption Whole blood clotting time Platelet function Clot formation: 4-8 min Clot formation abnormality indicates severe Fibrinolytic activity Clot retraction: <1 hr deficiency Clot lysis: none in 24 hr Abnormal retraction with thrombocytopenia Fibrinogen Fibrinogen level 400-650 mg/100 mL Usually decreased Platelet count Number of platelets >140,000/mm3 Usually decreased Fibrin degradation products Fibrin and fibrinogen <10 μg/mL Almost always elevated; most sensitive test degradation products Euglobulin clot lysis time Fibrinolytic activity None in 2 hr Difficult to interpret with low fibrinogen levels Prothrombin time Factors II, V, VII, X 10-12 sec Normal to prolonged Partial thromboplastin time Factors II, V, XIII, IX, X, XI 24-38 sec Normal to prolonged Thrombin time Factors I, II 16-20 sec Parallels fall in fibrinogen; good marker of Circulating split products abruption severity Heparin effect Red blood cell morphology Microangiopathic hemolysis Absence of distortion Presence of distortion or fragmentation is or fragmentation uncommon but indicates risk of renal cortical necrosis TABLE 37-4 BLOOD REPLACEMENT PRODUCTS Component Volume per Unit (mL)* Factors Present Effect of 1 Unit Fresh whole blood 500 RBCs; all procoagulants ↑ Hematocrit 3% Packed RBCs 200 RBCs only ↑ Hematocrit 3% Fresh-frozen plasma 200-400 All procoagulants; no platelets ↑ Fibrinogen 25 mg/dL Cryoprecipitate 20-50 Fibrinogen; factors VIII, XIII ↑ Fibrinogen 15-25% Platelet concentrate 35-60 Platelets; small amounts of fibrinogen; ↑ Platelet count approximately 8000/mm3 factors V, VIII RBCs, red blood cells. *Volume depends on individual blood bank.
- 10. 734 CHAPTER 37 Placenta Previa, Placenta Accreta, Abruptio Placentae, and Vasa Previa 21. Lauria MR, Smith RS, Treadwell MC, et al: The use of second-trimester Prevention transvaginal sonography to predict placenta previa. Ultrasound Obstet A prior abruption increases the risk of abruption in a subsequent Gynecol 8:337-340, 1996. pregnancy up to 20-fold.151 Modification of risk factors includes treat- 22. Dashe JS, McIntire DD, Ramus RM, et al: Persistence of placenta previa according to gestational age at ultrasound detection. Obstet Gynecol ment of chronic hypertension, smoking cessation, and avoidance of 99:692-697, 2002. substance abuse. Women with hyperhomocysteinemia should be 23. Ghourab S: Third-trimester transvaginal ultrasonography in placenta treated with folate. previa: Does the shape of the lower placental edge predict clinical outcome? Ultrasound Obstet Gynecol 18:103-108, 2001. 24. Cotton DB, Read JA, Paul RH, Quilligan EJ: The conservative aggressive management of placenta previa. Am J Obstet Gynecol 137:687-695, References 1980. 1. Ananth CV, Wilcox AJ, Savitz DA, et al: Effect of maternal age and parity 25. Love CD, Wallace EM: Pregnancies complicated by placenta praevia: What on the risk of uteroplacental bleeding disorders in pregnancy. Obstet is appropriate management? BJOG 103:864-867, 1996. Gynecol 88:511-516, 1996. 26. Brenner WE, Edelman DA, Hendricks CH: Characteristics of patients with 2. Iyasu S, Saftlas AK, Rowley DL, et al: The epidemiology of placenta previa placenta previa and results of “expectant management.” Am J Obstet in the United States, 1979 through 1987. Am J Obstet Gynecol 168:1424- Gynecol 132:180-191, 1978. 1429, 1993. 27. Towers CV, Pircon RA, Heppard M: Is tocolysis safe in the management 3. Frederiksen MC, Glassenberg R, Stika CS: Placenta previa: A 22-year of third-trimester bleeding? Am J Obstet Gynecol 180:1572-1578, 1999. analysis. Am J Obstet Gynecol 180:1432-1437, 1999. 28. Besinger RE, Moniak CW, Paskiewicz LS, et al: The effect of tocolytic use 4. Hemminki E, Merilainen J: Long-term effects of cesarean sections: Ectopic in the management of symptomatic placenta previa. Am J Obstet Gynecol pregnancies and placental problems. Am J Obstet Gynecol 174:1569-1574, 172:1770-1775; discussion 1775-1778, 1995. 1996. 29. Sharma A, Suri V, Gupta I: Tocolytic therapy in conservative management 5. Hershkowitz R, Fraser D, Mazor M, Leiberman JR: One or multiple previ- of symptomatic placenta previa. Int J Gynaecol Obstet 84:109-113, ous cesarean sections are associated with similar increased frequency of 2004. placenta previa. Eur J Obstet Gynecol Reprod Biol 62:185-188, 1995. 30. Droste S, Keil K: Expectant management of placenta previa: Cost-benefit 6. Monica G, Lilja C: Placenta previa, maternal smoking and recurrence risk. analysis of outpatient treatment. Am J Obstet Gynecol 170:1254-1257, Acta Obstet Gynecol Scand 74:341-345, 1995. 1994. 7. Timor-Tritsch IE, Yunis RA: Confirming the safety of transvaginal sonog- 31. Mouer JR: Placenta previa: Antepartum conservative management, inpa- raphy in patients suspected of placenta previa. Obstet Gynecol 81:742-744, tient versus outpatient. Am J Obstet Gynecol 170:1683-1685; discussion 1993. 1685-1686, 1994. 8. Williams MA, Mittendorf R: Increasing maternal age as a determinant of 32. Rosen DM, Peek MJ: Do women with placenta praevia without antepar- placenta previa: More important than increasing parity? J Reprod Med tum haemorrhage require hospitalization? Aust N Z J Obstet Gynaecol 38:425-428, 1993. 34:130-134, 1994. 9. Taylor VM, Kramer MD, Vaughan TL, Peacock S: Placenta previa and prior 33. Wing DA, Paul RH, Millar LK: Management of the symptomatic placenta cesarean delivery: How strong is the association? Obstet Gynecol 84:55-57, previa: A randomized, controlled trial of inpatient versus outpatient 1994. expectant management. Am J Obstet Gynecol 175:806-811, 1996. 10. Handler AS, Mason ED, Rosenberg DL, Davis FG: The relationship 34. D’Angelo LJ, Irwin LF: Conservative management of placenta previa: A between exposure during pregnancy to cigarette smoking and cocaine use cost-benefit analysis. Am J Obstet Gynecol 149:320-326, 1984. and placenta previa. Am J Obstet Gynecol 170:884-889, 1994. 35. Arias F: Cervical cerclage for the temporary treatment of patients with 11. Wexler P, Gottesfeld KR: Early diagnosis of placenta previa. Obstet Gynecol placenta previa. Obstet Gynecol 71:545-548, 1988. 54:231-234, 1979. 36. Cobo E, Conde-Agudelo A, Delgado J, et al: Cervical cerclage: An alterna- 12. Smith RS, Lauria MR, Comstock CH, et al: Transvaginal ultrasonography tive for the management of placenta previa? Am J Obstet Gynecol 179:122- for all placentas that appear to be low-lying or over the internal cervical 125, 1998. os. Ultrasound Obstet Gynecol 9:22-24, 1997. 37. Oppenheimer LW, Farine D, Ritchie JW, et al: What is a low-lying placenta? 13. Leerentveld RA, Gilberts EC, Arnold MJ, Wladimiroff JW: Accuracy and Am J Obstet Gynecol 165:1036-1038, 1991. safety of transvaginal sonographic placental localization. Obstet Gynecol 38. Bhide A, Prefumo F, Moore J, et al: Placental edge to internal os distance 76:759-762, 1990. in the late third trimester and mode of delivery in placenta praevia. BJOG 14. Rosati P, Guariglia L: Clinical significance of placenta previa detected at 110:860-864, 2003. early routine transvaginal scan. J Ultrasound Med 19:581-585, 2000. 39. Dawson WB, Dumas MD, Romano WM, et al: Translabial ultrasonogra- 15. Hertzberg BS, Bowie JD, Carroll BA, et al: Diagnosis of placenta previa phy and placenta previa: Does measurement of the os-placenta distance during the third trimester: Role of transperineal sonography. AJR Am J predict outcome? J Ultrasound Med 15:441-446, 1996. Roentgenol 159:83-87, 1992. 40. Royal College of Obstetricians and Gynaecologists. Placenta Praevia and 16. Oyelese Y, Smulian JC: Placenta previa, placenta accreta, and vasa previa. Placenta Praevia Accreta Diagnosis and Management. Clinical Green Top Obstet Gynecol 107:927-941, 2006. Guidelines No. 27. London, RCOG, 2005. 17. Becker RH, Vonk R, Mende BC, et al: The relevance of placental location 41. Boehm FH, Fleischer AC, Barrett JM: Sonographic placental localization at 20-23 gestational weeks for prediction of placenta previa at delivery: in the determination of the site of uterine incision for placenta previa. J Evaluation of 8650 cases. Ultrasound Obstet Gynecol 17:496-501, 2001. Ultrasound Med 1:311-314, 1982. 18. Taipale P, Hiilesmaa V, Ylostalo P: Transvaginal ultrasonography at 18-23 42. Lynch BC, Coker A, Lawal AH, et al: The B-Lynch surgical technique weeks in predicting placenta previa at delivery. Ultrasound Obstet Gynecol for the control of massive postpartum haemorrhage: An alternative to 12:422-425, 1998. hysterectomy? Five cases reported. BJOG 104:372-375, 1997. 19. Hill LM, Dinofrio DM, Chenevey P: Transvaginal sonographic evaluation 43. Bonner SM, Haynes SR, Ryall D: The anaesthetic management of caesar- of first-trimester placenta previa. Ultrasound Obstet Gynecol 5:301-303, ean section for placenta praevia: A questionnaire survey. Anaesthesia 1995. 50:992-994, 1995. 20. Mustafa SA, Brizot ML, Carvalho MH, et al: Transvaginal ultrasonography 44. Parekh N, Husaini SW, Russell IF: Caesarean section for placenta praevia: in predicting placenta previa at delivery: A longitudinal study. Ultrasound A retrospective study of anaesthetic management. Br J Anaesth 84:725- Obstet Gynecol 20:356-359, 2002. 730, 2000.
- 11. CHAPTER 37 Placenta Previa, Placenta Accreta, Abruptio Placentae, and Vasa Previa 735 45. Hong JY, Jee YS, Yoon HJ, Kim SM: Comparison of general and epidural 70. Spinillo A, Fazzi E, Stronati M, et al: Early morbidity and neurodevelop- anesthesia in elective cesarean section for placenta previa totalis: Maternal mental outcome in low-birthweight infants born after third trimester hemodynamics, blood loss and neonatal outcome. Int J Obstet Anesth bleeding. Am J Perinatol 11:85-90, 1994. 12:12-16, 2003. 71. Li DK, Wi S: Maternal placental abnormality and the risk of sudden infant 46. Usta IM, Hobeika EM, Musa AA, et al: Placenta previa-accreta: Risk factors death syndrome. Am J Epidemiol 149:608-611, 1999. and complications. Am J Obstet Gynecol 193:1045-1049, 2005. 72. Gielchinsky Y, Mankuta D, Rojansky N, et al: Perinatal outcome of preg- 47. Silver RM, Landon MB, Rouse DJ, et al: Maternal morbidity associated nancies complicated by placenta accrtea. Obstet Gynecol 104:527-530, with multiple repeat cesarean deliveries. Obstet Gynecol 107:1226-1232, 2004. 2006. 73. Fung TY, Lau TK: Poor perinatal outcome associated with vasa previa: Is 48. Clark SL, Koonings PP, Phelan JP: Placenta previa/accreta and prior cesar- it preventable? A report of three cases and review of the literature. Ultra- ean section. Obstet Gynecol 66:89, 1985. sound Obstet Gynecol 12:430-433, 1998. 49. Chattopadhyay SK, Kharif H, Sherbeeni MM: Placenta previa and accreta 74. Oyelese KO, Turner M, Lees C, Campbell S: Vasa previa: An avoidable after previous cesarean section. Eur J Obstet Gynaecol Reprod Biol 52:151, obstetric tragedy. Obstet Gynecol Surv 54:138-145, 1999. 1993. 75. Lijoi AF, Brady J: Vasa previa diagnosis and management. J Am Board Fam 50. Lira Plascencia J, Ibarguengoitia Ochoa F, Arqueta Z, et al: Placenta Pract 16:543-548, 2003. praevia/accreta and previous cesarean section: Experience of five years at 76. Francois K, Mayer S, Harris C, Perlow JH: Association of vasa previa at the Mexico National Institute of Perinatology. Gynecol Obstet Mex 63:337, delivery with a history of second-trimester placenta previa. J Reprod Med 1995. 48:771-774, 2003. 51. Rashbaum WK, Gates EJ, Jones J, et al: Placenta accreta encountered 77. Schachter M, Tovbin Y, Arieli S, et al: In vitro fertilization is a risk factor during dilation and evacuation in the second trimester. Obstet Gynecol for vasa previa. Fertil Steril 78:642-643, 2002. 85:701, 1995. 78. Antoine C, Young BK, Silverman F, et al: Sinusoidal fetal heart rate pattern 52. Comstock CH: Antenatal diagnosis of placenta accreta: A review. Ultra- with vasa previa in twin pregnancy. J Reprod Med 27:295-300, 1982. sound Obstet Gynecol 26:89-96, 2005. 79. Schellpfeffer MA: Improved neonatal outcome of vasa previa with aggres- 53. Warshak CR, Eskander R, Hull AD, et al: Accuracy of ultrasonography and sive intrapartum management: A report of two cases. J Reprod Med magnetic resonance imaging in the diagnosis of placenta accreta. Obstet 40:327-332, 1995. Gynecol 108:573-581, 2006. 80. Vandrie DM, Kammeraad LA: Vasa previa: Case report, review and 54. Grosvenor A, Silver R, Porter TF, et al: Optimal management of placenta presentation of a new diagnostic method. J Reprod Med 26:577-580, accreta. Am J Obstet Gynecol 195(6 Suppl 1):S82, 2006. 1981. 55. Levine D, Hulka CA, Ludmir J, et al: Placenta accreta: Evaluation with 81. Catanzarite V, Maida C, Thomas W, et al: Prenatal sonographic diagnosis color Doppler US, power Doppler US, and MI imaging. Radiology 205:773, of vasa previa: Ultrasound findings and obstetric outcome in ten cases. 1997. Ultrasound Obstet Gynecol 18:109-115, 2001. 56. Finberg HJ, Williams JW: Placenta accreta: Prospective sonographic diag- 82. Lee W, Lee VL, Kirk JS, et al: Vasa previa: Prenatal diagnosis, natural evolu- nosis in patients with placenta previa and previous cesarean section. J tion, and clinical outcome. Obstet Gynecol 95:572-576, 2000. Ultrasound Med 11:333-343, 1992. 83. Daly-Jones E, Hollingsworth J, Sepulveda W: Vasa praevia: Second 57. Maldjian C, Adam R, Pelosi M, et al: MRI appearance of placenta percreta trimester diagnosis using colour flow imaging. BJOG 103:284-286, and placenta accreta. Magn Reson Imaging 17:965-971, 1999. 1996. 58. Lerner JP, Deane S, Timor-Tritsch IE: Characterization of placenta accreta 84. Sepulveda W, Rojas I, Robert JA, et al: Prenatal detection of velamentous using transvaginal sonography and color Doppler imaging. Ultrasound insertion of the umbilical cord: A prospective color Doppler ultrasound Obstet Gynecol 5:198, 1995. study. Ultrasound Obstet Gynecol 21:564-569. 59. Twickler DM, Lucas MJ, Balis AB, et al: Color flow mapping for myome- 85. Nomiyama M, Toyota Y, Kawano H: Antenatal diagnosis of velamentous trial invasion in women with a prior cesarean delivery. J Matern Fetal Med umbilical cord insertion and vasa previa with color Doppler imaging. 9:330, 2000. Ultrasound Obstet Gynecol 12:426-429, 1998. 60. Chou MM, Tseng JJ, Ho ES, et al: Three dimensional color power Doppler 86. Oyelese Y, Catanzarite V, Prefumo F, et al: Vasa previa: The impact of pre- imaging in the assessment of uteroplacental neovascularization in pla- natal diagnosis on outcomes. Obstet Gynecol 103:937-942, 2004. centa previa increta/percreta. Am J Obstet Gynecol 185:1257, 2001. 87. Nimmo MJ, Kinsella D, Andrews HS: MRI in pregnancy: The diagnosis of 61. Zelop CM, Harlow BL, Frigoletto FD, et al: Emergency peripartum hys- vasa previa by magnetic resonance imaging. Bristol Med Chir J 103:12, terectomy. Am J Obstet Gynecol 168:1443-1448, 1993. 1988. 62. Kwee A, Bots ML, Visser GH, et al: Emergency peripartum hysterectomy: 88. Canterino JC, Mondestin-Sorrentino M, Muench MV, et al: Vasa previa: A prospective study in the Netherlands. Eur J Obstet Gynecol Reprod Biol Prenatal diagnosis and evaluation with 3-dimensional sonography and 124:187-192, 2006. power angiography. J Ultrasound Med 24:721-724, quiz 725; 2005. 63. Bodner LJ, Nosher JL, Gribbin C, et al: Balloon-assisted occlusion of the 89. Oyelese Y, Chavez MR, Yeo L, et al: Three-dimensional sonographic diag- internal iliac arteries in patients with placenta accrete/percreta. Cardiovasc nosis of vasa previa. Ultrasound Obstet Gynecol 24:211-215, 2004. Intervent Radiol 29:354-361, 2006. 90. Ananth CV, Berkowitz GS, Savitz DA, Lapinski RH: Placental abruption 64. Shrivastava V, Nageotte M, Major C, et al. Case-control comparison of and adverse perinatal outcomes. JAMA 282:1646-1651, 1999. cesarean hysterectomy with and without prophylactic placement of intra- 91. Ananth CV, Wilcox AJ: Placental abruption and perinatal mortality in the fascular balloon catheters for placenta accreta. Am J Obstet Gynecol United States. Am J Epidemiol 153:332-337, 2001. 197:40231-40235, 2007. 92. Salihu HM, Bekan B, Aliyu MH, et al: Perinatal mortality associated with 65. Jaffe R, DuBeshter B, Sherer DM, et al: Failure of methotrexate treatment abruptio placenta in singletons and multiples. Am J Obstet Gynecol for term placenta percreta. Am J Obstet Gynecol 171:558, 1994. 193:198-203, 2005. 66. Matthews NM, McCowan LM, Patten P: Placenta previa accreta with 93. Rasmussen S, Irgens LM, Bergsjo P, Dalaker K: The occurrence of placental delayed hysterectomy. Aust N Z J Obstet Gynaecol 36:476, 1996. abruption in Norway 1967-1991. Acta Obstet Gynecol Scand 75:222-228, 67. Mussalli GM, Shah J, Berch DJ, et al: Placenta accreta and methotrexate 1996. therapy: Three case reports. J Perinatal 20:331, 2000. 94. Pritchard JA, Mason R, Corley M, Pritchard S: Genesis of severe placental 68. Varma TR: Fetal growth and placental function in patients with placenta abruption. Am J Obstet Gynecol 108:22-27, 1970. praevia. J Obstet Gynaecol Br Commonw 80:311-315, 1973. 95. Ananth CV, Oyelese Y, Yeo L, et al: Placental abruption in the United States, 69. Crane JM, van den Hof MC, Dodds L, et al: Neonatal outcomes with pla- 1979 through 2001: Temporal trends and potential determinants. Am J centa previa. Obstet Gynecol 93:541-544, 1999. Obstet Gynecol 192:191-198, 2005.
- 12. 736 CHAPTER 37 Placenta Previa, Placenta Accreta, Abruptio Placentae, and Vasa Previa 96. Oyelese Y, Ananth CV: Placental abruption. Obstet Gynecol 108:1005- 120. Addis A, Moretti ME, Ahmed Syed F, et al: Fetal effects of cocaine: An 1016, 2006. updated meta-analysis. Reprod Toxicol 15:341-369, 2001. 97. Perlman JM, Risser R: Can asphyxiated infants at risk for neonatal seizures 121. Hoskins IA, Friedman DM, Frieden FJ, et al: Relationship between ante- be rapidly identified by current high-risk markers? Pediatrics 97:456-462, partum cocaine abuse, abnormal umbilical artery Doppler velocimetry, 1996. and placental abruption. Obstet Gynecol 78:279-282, 1991. 98. Gibbs JM, Weindling AM: Neonatal intracranial lesions following placen- 122. Kupferminc MJ, Eldor A, Steinman N, et al: Increased frequency of genetic tal abruption. Eur J Pediatr 153:195-197, 1994. thrombophilia in women with complications of pregnancy. N Engl J Med 99. Spinillo A, Fazzi E, Stronati M, et al: Severity of abruptio placentae and 340:9-13, 1999. neurodevelopmental outcome in low birth weight infants. Early Hum Dev 123. Goddijn-Wessel TA, Wouters MG, van de Molen EF, et al: Hyperhomo- 35:45-54, 1993. cysteinemia: A risk factor for placental abruption or infarction. Eur J 100. Naeye RL, Harkness WL, Utts J: Abruptio placentae and perinatal death: Obstet Gynecol Reprod Biol 66:23-29, 1996. A prospective study. Am J Obstet Gynecol 128:740-746, 1977. 124. Prochazka M, Happach C, Marsal K, et al: Factor V Leiden in pregnancies 101. Rosen T, Schatz F, Kuczynski E, et al: Thrombin-enhanced matrix metal- complicated by placental abruption. BJOG 110:462-466, 2003. loproteinase-1 expression: A mechanism linking placental abruption with 125. Dizon-Townson D, Miller C, Sibai B, et al: The relationship of the factor premature rupture of the membranes. J Matern Fetal Neonatal Med 11:11- V Leiden mutation and pregnancy outcomes for mother and fetus. Obstet 17, 2002. Gynecol 106:517-524, 2005. 102. Hibbard BM, Jeffcoate TN: Abruptio placentae. Obstet Gynecol 27:155- 126. Jaaskelainen E, Keski-Nisula L, Toivonen S, et al: MTHFR C677T poly- 167, 1966. morphism is not associated with placental abruption or preeclampsia in 103. Sheiner E, Shoham-Vardi I, Hallak M, et al: Placental abruption in term Finnish women. Hypertens Pregnancy 25:73-80, 2006. pregnancies: Clinical significance and obstetric risk factors. J Matern Fetal 127. Jarvenpaa J, Pakkila M, Savolainen ER, et al: Evaluation of factor V Leiden, Neonatal Med 13:45-49, 2003. prothrombin and methylenetetrahydrofolate reductase gene mutations 104. Ananth CV, Smulian JC, Srinivas N, et al: Risk of infant mortality among in patients with severe pregnancy complications in northern Finland. twins in relation to placental abruption: Contributions of preterm birth Gynecol Obstet Invest 62:28-32, 2006. and restricted fetal growth. Twin Res Hum Genet 8:524-531, 2005. 128. Dahmus MA, Sibai BM: Blunt abdominal trauma: Are there any predictive 105. Dugoff L, Hobbins JC, Malone FD, et al: First-trimester maternal serum factors for abruptio placentae or maternal-fetal distress? Am J Obstet PAPP-A and free-beta subunit human chorionic gonadotropin concentra- Gynecol 169:1054-1059, 1993. tions and nuchal translucency are associated with obstetric complications: 129. Towery R, English TP, Wisner D: Evaluation of pregnant women after A population-based screening study (the FASTER Trial). Am J Obstet blunt injury. J Trauma 35:731-735; discussion 735-736, 1993. Gynecol 191:1446-1451, 2004. 130. Major CA, de Veciana M, Lewis DF, Morgan MA: Preterm premature 106. Dommisse J, Tiltman AJ: Placental bed biopsies in placental abruption. rupture of membranes and abruptio placentae: Is there an association BJOG 99:651-654, 1992. between these pregnancy complications? Am J Obstet Gynecol 172:672- 107. Harrington K, Cooper D, Lees C, et al: Doppler ultrasound of the uterine 676, 1995. arteries: The importance of bilateral notching in the prediction of pre- 131. Ball RH, Ade CM, Schoenborn JA, Crane JP: The clinical significance of eclampsia, placental abruption or delivery of a small-for-gestational-age ultransonographically detected subchorionic hemorrhages. Am J Obstet baby. Ultrasound Obstet Gynecol 7:182-188, 1996. Gynecol 174:996-1002, 1996. 108. Toivonen S, Heinonen S, Anttila M, et al: Obstetric prognosis after pla- 132. Yaron Y, Ochshorn Y, Heifetz S, et al: First trimester maternal serum free cental abruption. Fetal Diagn Ther 19:336-341, 2004. human chorionic gonadotropin as a predictor of adverse pregnancy 109. Ananth CV, Savitz DA, Williams MA. Placental abruption and its associa- outcome. Fetal Diagn Ther 17:352-356, 2002. tion with hypertension and prolonged rupture of membranes: A meth- 133. Pilalis A, Souka AP, Antsaklis P, et al: Screening for pre-eclampsia and fetal odologic review and meta-analysis. Obstet Gynecol 88:309-318, 1996. growth restriction by uterine artery Doppler and PAPP-A at 11-14 weeks’ 110. Golditch IM, Boyce NE Jr: Management of abruptio placentae. JAMA gestation. Ultrasound Obstet Gynecol 29:135-140, 2007. 212:288-293, 1970. 134. Katz VL, Chescheir NC, Cefalo RC: Unexplained elevations of maternal 111. Cnattingius S: Maternal age modifies the effect of maternal smoking on serum alpha-fetoprotein. Obstet Gynecol Surv 45:719-726, 1990. intrauterine growth retardation but not on late fetal death and placental 135. Jauniaux E, Gulbis B, Tunkel S, et al: Maternal serum testing for alpha- abruption. Am J Epidemiol 145:319-323. fetoprotein and human chorionic gonadotropin in high-risk pregnancies. 112. Kramer MS, Usher RH, Pollack R, et al: Etiologic determinants of abruptio Prenat Diagn 16:1129-1135, 1996. placentae. Obstet Gynecol 89:221-226, 1997. 136. Tikkanen M, Hamalainen E, Nuutila M, et al: Elevated maternal second- 113. Castles A, Adams EK, Melvin CL, et al: Effects of smoking during preg- trimester serum alpha-fetoprotein as a risk factor for placental abruption. nancy: Five meta-analyses. Am J Prev Med 16:208-215, 1999. Prenat Diagn 27:240-243, 2007. 114. Ananth CV, Savitz DA, Luther ER: Maternal cigarette smoking as a risk 137. Van Rijn M, van der Schouw YT, Hagenaars AM, et al: Adverse obstetric factor for placental abruption, placenta previa, and uterine bleeding in outcome in low- and high- risk pregnancies: Predictive value of maternal pregnancy. Am J Epidemiol 144:881-889, 1996. serum screening. Obstet Gynecol 94:929-934, 1999. 115. Ananth CV, Smulian JC, Vintzileos AM: Incidence of placental abruption 138. Towner D, Gandhi S, El Kady D: Obstetric outcomes in women with ele- in relation to cigarette smoking and hypertensive disorders during preg- vated maternal serum human chorionic gonadotropin. Am J Obstet nancy: A meta-analysis of observational studies. Obstet Gynecol 93:622- Gynecol 194:1676-1681; discussion 1681-1682, 2006. 628, 1999. 139. Nyberg DA, Mack LA, Benedetti TJ, et al: Placental abruption and placen- 116. Raymond EG, Mills JL: Placental abruption: Maternal risk factors and tal hemorrhage: Correlation of sonographic findings with fetal outcome. associated fetal conditions. Acta Obstet Gynecol Scand 72:633-639, Radiology 164:357-361, 1987. 1993. 140. Glantz C, Purnell L: Clinical utility of sonography in the diagnosis 117. Kyrklund-Blomberg NB, Gennser G, Cnattingius S: Placental abruption and treatment of placental abruption. J Ultrasound Med 21:837-840, and perinatal death. Paediatr Perinat Epidemiol 15:290-297, 2001. 2002. 118. Misra DP, Ananth CV: Risk factor profiles of placental abruption in first 141. Sholl JS: Abruptio placentae: Clinical management in nonacute cases. Am and second pregnancies: Heterogeneous etiologies. J Clin Epidemiol J Obstet Gynecol 156:40-51, 1987. 52:453-461, 1999. 142. Jaffe MH, Schoen WC, Silver TM, et al: Sonography of abruptio placentae. 119. Kennare R, Heard A, Chan A: Substance use during pregnancy: Risk AJR Am J Roentgenol 137:1049-1054, 1981. factors and obstetric and perinatal outcomes in South Australia. Aust N 143. Nyberg DA, Cyr DR, Mack LA, et al: Sonographic spectrum of placental Z J Obstet Gynaecol 45:220-225, 2005. abruption. AJR Am J Roentgenol 148:161-164, 1987.
- 13. CHAPTER 37 Placenta Previa, Placenta Accreta, Abruptio Placentae, and Vasa Previa 737 144. Warner MW, Salfinger SG, Rao S, et al: Management of trauma during 148. Bond AL, Edersheim TG, Curry L, et al: Expectant management of abrup- pregnancy. Aust N Z J Surg 74:125-128, 2004. tio placentae before 35 weeks gestation. Am J Perinatol 6:121-123, 1989. 145. Emery CL, Morway LF, Chung-Park M, et al: The Kleihauer-Betke test: 149. Combs CA, Nyberg DA, Mack LA, et al: Expectant management after Clinical utility, indication, and correlation in patients with placental sonographic diagnosis of placental abruption. Am J Perinatol 9:170-174, abruption and cocaine use. Arch Pathol Lab Med 119:1032-1037, 1992. 1995. 150. Saller DN Jr, Nagey DA, Pupkin MJ, Crenshaw MC Jr: Tocolysis in the 146. Elliott JP, Gilpin B, Strong TH Jr, Finberg HJ: Chronic abruption-oligo- management of third trimester bleeding. J Perinatol 10:125-128, 1990. hydramnios sequence. J Reprod Med 43:418-422, 1998. 151. Rasmussen S, Irgens LM, Dalaker K: Outcome of pregnancies subsequent 147. Knab DR. Abruptio placentae: An assessment of the time and method of to placental abruption: A risk assessment. Acta Obstet Gynecol Scand delivery. Obstet Gynecol 52:625-629, 1978. 79:496-501, 2000.