Pelvic, Hip and Core Stability
•
16 gefällt mir•9,357 views

Pelvic, Hip and Core Stability From Grégoire Lason and Luc Peeters, The International Academy of Osteopathy, www.osteopathy.eu Also visit: http://www.osteoapps.eu - A must have for every osteopath and health care provider. Simple to use and no unnecessary information. It keeps your knowledge sharp for daily patient care! Also look for iBooks in the iBook store from Luc Peeters and Grégoire Lason.

Empfohlen
Weitere ähnliche Inhalte
Was ist angesagt?
Was ist angesagt? (20)
Andere mochten auch
Andere mochten auch (20)
Ähnlich wie Pelvic, Hip and Core Stability
Ähnlich wie Pelvic, Hip and Core Stability (20)
Mehr von IAO The International Academy of Osteopathy
Mehr von IAO The International Academy of Osteopathy (14)
Kürzlich hochgeladen
Kürzlich hochgeladen (20)
Pelvic, Hip and Core Stability
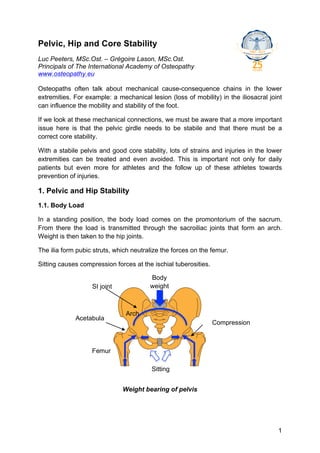
- 1. Pelvic, Hip and Core Stability Luc Peeters, MSc.Ost. – Grégoire Lason, MSc.Ost. Principals of The International Academy of Osteopathy www.osteopathy.eu Osteopaths often talk about mechanical cause-consequence chains in the lower extremities. For example: a mechanical lesion (loss of mobility) in the iliosacral joint can influence the mobility and stability of the foot. If we look at these mechanical connections, we must be aware that a more important issue here is that the pelvic girdle needs to be stabile and that there must be a correct core stability. With a stabile pelvis and good core stability, lots of strains and injuries in the lower extremities can be treated and even avoided. This is important not only for daily patients but even more for athletes and the follow up of these athletes towards prevention of injuries. 1. Pelvic and Hip Stability 1.1. Body Load In a standing position, the body load comes on the promontorium of the sacrum. From there the load is transmitted through the sacroiliac joints that form an arch. Weight is then taken to the hip joints. The ilia form pubic struts, which neutralize the forces on the femur. Sitting causes compression forces at the ischial tuberosities. Body SI joint weight Arch Acetabula Compression Femur Sitting Weight bearing of pelvis 1
- 2. Pelvic ring In a standing position, the sacrum is loaded with the superincumbent weight. Primary vertebral load on the sacral promontorium causes the sacrum to rotate anterior. This is called primary load on S1. The posterior sacroiliac capsule takes the tensile stress. This causes the caudal part of the sacrum to move posteriorly causing a counter-balancing tensile stress on the sacrospinous and sacrotuberous ligaments. Relatively, the iliac bones rotate posteriorly. The weight bearing forces join at the inferior transverse axis. Under load, the sacrum tilts anterior. The more load, the more anterior tilt of the sacrum. This induces the lumbar spine in more lordosis. This caudal gravity load on the sacrum with tensile stretch on the posterior capsule and the sacrospinous- and sacrotuberous ligaments happens around the ITA, thus compressing the inferior part of the SI joints lateromedially on this S3 level. Primary load force at S1 40° ITA (L3 level) Compression at S3 level = self-bracing 10° Sacrum in weight bearing (redrawn from Vleeming) 2
- 3. On the cephalic side of S3 (on the iliac bone) there is an ilial ridge. This prevents S3 to move cranially. Ilial ridge ITA (L3 level) Ilial ridge postero-superior from the ITA After load bearing, the gravity line is anterior to the sacral axis. The gravity line stays posterior to the acetabula causing a general posterior pelvic tilt and creating a dynamic, balanced tension on the pelvic ligaments. The posterior pelvic tilt decreases the lumbar lordosis. The ligamentary stability of the pelvis in the sagittal plane is maintained by a good condition of the posterior sacroiliac capsule and the sacrospinous- and sacrotuberous ligaments. The basic muscular balance is done by the lower paravertebral muscles and the coccygeal muscles. Secondary the piriformis m. and the sacral part of the gluteus maximus m. provide a counter force for the anterior sacral rotation. Posterior sacroiliac capsule and lower paravertebral muscles Sacrospinous, sacrotuberous ligaments and coccygeal muscles Ligamentary stability and muscular balance in the sagittal plane 3
- 4. To have an optimal functioning pelvic girdle that spreads tension equally over the joints and capsuloligamentary structures, the correct locking mechanism (self- bracing) must be in place. Therefore the condition of the posterior SI capsule and sacrospinous- and tuberous ligaments must be optimal. Despite good condition of these ligamentary structures, they are not sufficient to maintain a good self-bracing, thus keeping the appearance of lesions to a minimum. There is also a need for a good functioning muscular system that maintains the self- bracing mechanism intact. Three muscle slings (chains) are supposed to contribute to force closure of the SI joints: • A longitudinal muscle sling. • A posterior oblique muscle sling. • An anterior oblique muscle sling. The longitudinal muscle sling consists of the combination of the low paravertebral muscles attaching to the sacrum, the deep layer of the thoracolumbar fascia and the sacrotuberous ligament, which is connected to the long head of the biceps femoris muscle. Tension in this muscle sling will stabilize the SI joint in 3 ways: • Contraction of the low paravertebral muscles will anteriorize the sacrum. This increased the tension on the posterior SI capsule thus leading to more force closure of the SI joints. • Contraction of these muscles will also inflate the thoracolumbar fascia leading to more force closure. • Due to the anatomical relation with the sacrotuberous ligament, the contraction of these muscles will increase tension on the ligament thus increasing the closure of the SI joint. 4
- 5. Paravertebral muscles + thoracolumbar fascia Sacrospinous- and sacrotuberal ligs. Biceps femoris m. Longitudinal muscle sling The posterior oblique sling is the coupled function of the latissimus dorsi muscle and the gluteus maximus muscle. Both muscles function as synergists. Contraction will directly optimize stabilization of the SI joints. 5
- 6. Latissimus dorsi m. Gluteus maximus m. Left Right Posterior oblique sling The anterior oblique sling consists of the external and internal oblique muscles as well as of the transverse abdominis muscle (connection via rectus sheet). Muscle contraction of this sling also increases the SI stabilization (self-bracing mechanism). External and internal oblique m., transverse abdominis m. Right Left Anterior oblique sling For example sitting with the legs crossed reduces strongly the tone of the anterior oblique sling. This is because sitting with crossed legs increases mechanically the SI compression and friction. Reducing this muscle tone diminishes this compression and friction. A good stability of pelvis and hips means: • Line of gravity between the inferior transverse axis of the SI joint and the acetabula. • Good, harmonious ligamentary tension. 6
- 7. • Good harmonious muscular balance. • Correct anatomical angulation of the hip. Secondary load force at S3 Posterior pelvic (ilial) tilt around the hip Anterior sacrum tilt around the ITA Gravity line and weight balance 1.2. The Hip The capsular thickenings form a spiral around the hip. In extension these fibres become taut with the result that the head of the femur is held securely in the acetabulum and the joint becomes "locked" or "close-packed" - the position of maximum stability and firmness for the hip. All the major joints (hip, knee, ankle) become close-packed at full extension and this coincides with the limb becoming a rigid, vertical, weight-bearing pillar. This is clearly the essential prerequisite for standing upright on two legs i.e. the adoption of bipedal stance. When standing erect the centre of gravity passes behind the hip joint. This should result in hyperextension at the hip. It is especially the iliofemoral lig. that withstands this extension. 7
- 8. Iliofemoral lig. withstanding extension in standing position 1.3. Leg Length Difference If there is an anatomical leg length difference, the left and right ligamentary tension is different. Although the body can compensate, this anatomical leg length difference will reduce the stability and mechanical resistance to avoid lesions. Not every leg length difference however is anatomical. A pelvic torsion can cause an apparent leg length difference. Importance of hip- and pelvic stability: they are the basis for the core stability. 2. Core Stability Core stability means the ability of the lumbo-pelvic-hip complex to prevent buckling of the vertebral column and to return it to equilibrium following perturbation. Coordination and co-contraction of muscles provide spine stiffness. In other words “it is the ability to control the position and motion of the trunk over the pelvis to allow optimum production, transfer and control of force and motion to the terminal segment in integrated kinetic chain activities”. (Kibler et al 2006) Core stability can also be described as the possibility to continually and instantaneous adapt to changing postures and loading conditions. It ensures the integrity of the spine and provides a stable base for the movements of the extremities. The core also absorbs forces transmitted through the lower extremity during activity. The hip and the lower extremity can be seen as mobile structures but the mobility of extremity movements depends on the core activity. Core muscles are active before the initiation of extremity movements. “Proximal stability before distal mobility”. 8
- 9. “Core stability may provide several benefits to the musculoskeletal system, from maintaining low back health to preventing knee injury” (Willson et al 2005). Core stability in practice: 1. Lumbo-pelvic-hip complex: good symmetrical mobility and local hip and pelvic stability. 2. Good muscular balance (in length, tone and strength) in the three planes: a. In the sagittal plane: i. Rectus abdominis m. ii. Transverse abdominis m. iii. Erector spinae m. iv. Multifidus m. v. Gluteus max. m. vi. Hamstrings. vii. Co-contraction of these muscles causes trunk stiffness, raises the intra-abdominal pressure and provides a stable core. b. In the frontal plane: i. Glut med., glut min. m. ii. Quadratus lumborum m. iii. Hip adductors. c. In the transverse plane: i. Hip rotators. ii. Trunk rotators 3. Stabilizing corset effect of the thoracolumbar fascia. Abdominals 9
- 10. Quadratus lumborum m. Erector trunci Transverse Gluteus med. & abdominis m. min. m. Rectus abdominis Gluteus max. m. Adductors Hamstrings In the sagittal plane In the frontal plane Obliquus internus and externus Hip rotators In the horizontal plane A poor core function/stability can be caused by: • Lesion in the hip, pelvic and low lumbar joints. • Muscular weakness and/or disbalance. • Poor muscular endurance. • Fatigue. • Pain/injury – avoidance. When during activity, the muscles cannot stabilize the spine, pelvis and hips (core), the patient will be vulnerable for injury. 10
- 11. To illustrate this: it is recently found that patients with paravertebral muscular dysfunction show increased quadriceps inhibition. (Hart et al 2005). The osteopath therefore will always evaluate the patients’ core stability by: • Testing the hip, pelvis and low lumbar joints for harmonious mobility. • Testing for equal capsuloligamentary tension. • Testing the muscular balance in the three planes (on length, tone and strength). 3. Bibliography Byrne D.P., Mulhall K.J. & Baker J.F. (2010) Anatomy & Biomechanics of the Hip. The Open Sports Medicine Journal, Vol. 4, pp. 51-57. Campbell J.D., Higgs R., Wright K. & Leaver-Dunn D. (2001) Pelvis, hip and thigh injuries. In: Schenck R.C., Guskiewicz K.M., Holmes C.F., Eds. Athletic Training and Sports Medicine. Rosemount: American Academy of Orthopaedic Surgeons; p. 399. DonTigny R. (1993) Mechanics and Treatment of the Sacroiliac Joint, The Journal of Manual and Manipulative Therapy. Vol.1, No. 1, pp. 3-12. DonTigny R.L. (1994) Function of the Lumbosacroiliac complex as a self- compensating force couple with a variable, force-depending transverse axis: A theoretical analysis. The Journal of Manual dz Manipulative Therapy 2: 87-93. DonTigny R.L. (2005) Critical analysis of the functional dynamics of the sacroiliac joints as they pertain to normal gait. J of Orthopaedic Medicine (UK) 27:3-10. DonTigny R.L. (2007) A detailed and critical biomechanical analysis of the sacroiliac joints and relevant kinesiology. The implications for lumbopelvic function and dysfunction. In Vleeming A, Mooney V, and Stoeckart R (eds): Movement, Stability & Lumbopelvic Pain: Integration of Research and Therapy. Churchill Livingstone, 2 edition, Chapter 18, pp 265-278. Gracovetsky S. (2007) Stability or controlled instability? In Vleeming A, Mooney V, and Stoeckart R (eds): Movement, Stability & Lumbopelvic Pain: Integration of Research and Therapy. Churchill Livingstone, 2 edition, Chapter 19, pp 278-294. Hart D.L., Stobbe T.J., Till C.W. & Plummer R.W. (2005) Effect of Trunc Stabilization on Quadriceps Muscle Torque. West Virginia University, Morgastown. Hart J.M., Kerrigan D.C., Fritz J.M., Saliba E.N., Gansneder B. & Ingersoll C.D. (2005) Contribution of Hamstrings fatigue to quadriceps inhibition following lumbar extension exercise. Journal of Sports Science and Medicine (2006) 5, 70-79. Kibler W.B., Press J., & Sciascia A. (2006) The role of core stability in athletic function. Sports Med, 2006. 36(3): 189-198. 11
- 12. Lee D. et Vleeming A. (2004) The management of pelvic joint pain & dysfunction. Chapter 34 in Grieves Modern Manual Therapy: The vertebral column. Churchill Livingstone, Edinburgh. P. 495-506. Leetun D.T., Ireland M.L., Willson J.D., Ballantyne B.T., & Davis I.M. (2004) Core stability measures as risk factors for lower extremity injury in athletes. Med Sci Sports Exerc. 36(6): 926-934. Peeters L. & Lason G. (2005) Integratie en toegepaste principes in de Osteopathie – Osteo 2000. (Ed.). Vleeming A. et al (1990) Relation between Form and Function in the Sacroiliac Joint Part I & Part II Spine 15(2): pp. 30–135. Vleeming A., van Wingerden J.P., & Dijkstra P.F. (1992) Mobility in the sacroiliac joints in the elderly: a kinematic and radiological study. Clin Biomech;7:170–176. Vleeming A., Mooney V., Dorman T., Snijders, Stoeckart R. (1995) The Function of the Lumbar Spine and Sacroiliac Joint Part I and II. Rotterdam Philips. Vleeming A., Pool-Goudzwaard A., Hammudoghlu D., Stoeckart R., Snijders C. & mens J.M.A. (1996) The Function of the Long Dorsal Sacroiliac Ligament. Its implication for Understanding Low Back Pain. Spine. Volume 21. Number 5. pp. 556- 562. Vleeming A., Mooney V., Dorman T., Snijders C. & Stoeckart R., (1997) Movement Stability and Low Back Pain. The Essential Role of the Pelvis. Edinburgh, Churchill Livingstone. Vleeming A., de Vries J.H.J., Mens J.M., & van Wingerden J.P. (2002) Possible role of the long dorsal sacroiliac ligament in women with peripartum pelvic pain. Acta Obstet. Gynecol. Scand. 81(5): 430-436. Willson J.D., Dougherty C.P., Ireland M.L., & Davis I.M. (2005) Core stability and its relationship to lower extremity function and injury. J Am Acad Orthop Surg. 13(5): 316-325. http://www.facebook.com/IAOdeutsch All rights reserved. © 2012. http://www.facebook.com/IAOenglish No part of this article may be http://www.facebook.com/IAOnederlands reproduced or made public by http://www.facebook.com/IAOfrancais printing, photocopying, microfilming, or by any means without the prior written permission of the publisher. iNeuro APP iCranialNerves APP 12